"Purchase cheap lurantal line, acne scar removal."By: Joshua C Briscoe, MD - Medical Instructor in the Department of Psychiatry and Behavioral Sciences
- Medical Instructor in the Department of Medicine
 https://medicine.duke.edu/faculty/joshua-c-briscoe-md
Buy generic lurantal 10 mg onlineCatecholamines are launched in response to decreased glucose concentrations, varied types of stress, and exercise. The direct metabolic actions of catecholamines are mediated primarily by 1-, 2-, and 3-adrenergic receptors located on muscle, adipose, and liver tissue (see later). Hormonal Regulation of Specific Metabolic Reactions and Pathways this part discusses the principle pathways in hepatocytes, skeletal myocytes, and adipocytes that contribute to built-in metabolism. For much more detailed description, the coed is referred to biochemistry textbooks. Fasting Phases Some of the necessary thing metabolic steps regulated by insulin and glucagon (and catecholamines) within the liver are as follows (refer to . Insulin prevents the futile cycle of glucose phosphorylation-dephosphorylation by repressing gene expression of the enzyme G6Pase. Insulin not directly increases glycogen synthesis by way of elevated expression of glucokinase because high ranges of G6P allosterically increase glycogen synthase activity. Through stimulation of specific protein phosphatases, insulin promotes dephosphorylation and thereby activation of glycogen synthase (reaction 2D). Insulin additionally prevents the futile cycle of glycogen synthesis to glycogenolysis through inhibition of glycogen phosphorylase (reaction 2F). Insulin also inhibits the reverse reaction, as catalyzed by the gluconeogenic enzyme fructose-1,6-bisphosphatase. F-2,6-bisP also competitively inhibits fructose-1,6bisphosphatase, thereby blocking the futile cycle of F6P to fructose-1,6-bisphosphate to F6P. The first step includes conversion of acetyl CoA to malonyl CoA by the enzyme acetyl-CoA carboxylase (reaction 9D). Insulin additionally promotes dephosphorylation of acetyl-CoA carboxylase, which activates the enzyme. Glucagon also phosphorylates and prompts the enzyme malonyl decarboxylase, which converts malonyl CoA back to acetyl CoA (reaction 9F). Glucose tolerance refers to the flexibility of an individual to decrease the increase in blood glucose concentration after a meal. A main way by which insulin promotes glucose tolerance is activation of glucose transporters in skeletal muscle. Insulin additionally promotes storage of glucose in muscle as glycogen (reaction 2D) and promotes oxidation of glucose by way of glycolysis (reaction 3D). Exercise additionally activates these pathways, as does glycogenolysis (reaction 2F), by way of adrenergic receptor stimulation. B, Lipid metabolism in adipocyte throughout digestive ("D" reactions) and fasting ("F" reactions) phases. In the absence of insulin these two merchandise of lipolysis are exported into the blood. There are also "remnants" of lipoproteins which have their lipid cargo partially digested and then cleared from the circulation by the liver. Chylomicrons are secreted, move into lymphatics, and then ultimately enter the circulation. This means of adipocyte differentiation, which can proceed throughout life, is promoted by a number of transcription elements. Leptin Leptin is an adipocyte-derived protein that alerts data to the hypothalamus about the diploma of adiposity and diet, which in turn controls eating conduct and power expenditure. These findings originally raised hope that leptin therapy could be used to combat morbid weight problems. In reality, obese individuals have already got elevated endogenous circulating ranges of leptin and appear to have developed leptin resistance. This motion of leptin, although opposing the lipogenic actions of insulin, contributes considerably to upkeep of insulin sensitivity (as outlined by insulin-dependent glucose uptake) in peripheral tissues. Leptin additionally acts as a sign that the body has sufficient vitality shops to enable replica and to enhance erythropoiesis, lymphopoiesis, and myelopoiesis. For example, in girls affected by anorexia nervosa, leptin levels are extraordinarily low and result in low ovarian steroids, amenorrhea (lack of menstrual bleeding), anemia from low red blood cell manufacturing, and immune dysfunction. Structure, Synthesis, and Secretion Leptin, a 16-kDa protein secreted by mature adipocytes, is structurally related to cytokines. Circulating ranges of leptin have a direct relationship with adiposity and nutritional status. Leptin output is increased by insulin, which prepares the body for correct partitioning of incoming nutrients. Energy Storage the amount of energy stored by an individual is decided by caloric intake and calories expended as energy per day. In many people, input and output are in steadiness, so weight remains comparatively fixed. In addition, the gestational environment has a profound impact on body mass of the adult. The impact of maternal food plan on the weight and body composition of offspring known as fetal programming. Low start weights correlate with elevated threat for weight problems, cardiovascular disease, and diabetes. These findings suggest that the efficiency of fetal metabolism has plasticity and can be altered by the in utero setting. The situation of being chubby or obese is a risk issue for a number of pathologies, including insulin resistance, dyslipidemia, diabetes, cardiovascular disease, and hypertension. These depots obtain different blood supplies which are drained in a basically completely different means in that venous return from intraabdominal fats leads into the hepatic portal system. Abdominal fats is extremely innervated by autonomic neurons and has a larger turnover rate. Furthermore, these two depots display variations in hormone production and enzyme exercise. Men are inclined to gain fats in the intraabdominal depot (android [apple-shaped] adiposity), whereas ladies are most likely to achieve fat within the subcutaneous depot, particularly within the thighs and buttocks (gynecoid [pear-shaped] adiposity). Clearly an excess of stomach fats poses a greater risk factor for the pathologies mentioned earlier. Thus another indicator of body composition is circumference of the waist (measured in inches across the narrowest point between the ribs and hips when considered from the entrance after exhaling) divided by the circumference of the hips (measured on the point where the buttocks are largest when seen from the side). Central Mechanisms Involved in Energy Balance In current years, numerous hormones and neuropeptides have been implicated in both continual and acute regulation of appetite, satiety, and vitality expenditure in humans. Leptin acts on no less than two neuron types in the arcuate nucleus of the hypothalamus. These second-order neuropeptides are transmitted to and interact with receptors in neurons of the paraventricular hypothalamic nucleus ("satiety" neurons) and lateral hypothalamic nucleus ("hunger" neurons). In flip these hypothalamic neurons generate indicators that coordinate feeding conduct and autonomic nervous system exercise (especially sympathetic outflow) with numerous endocrine actions on thyroid gland function, copy, and progress. To keep total power homeostasis, the system should also stability specific nutrient consumption and expenditure-for instance, carbohydrate consumption with carbohydrate oxidation.
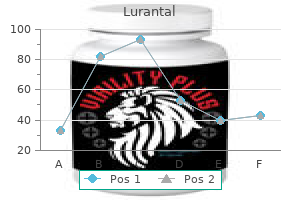
Safe 5mg lurantalAt any given degree of ventricular filling, the slope supplies an index of the preliminary contraction velocity and therefore an index of contractility. A(blue curve),management; B (dashed pink curve), hyperdynamic coronary heart, as with administration of norepinephrine; C (green dashed curve), hypodynamic heart, as in cardiacfailure. In addition, the ejection fraction, which is the ratio of the quantity of blood ejected from the left ventricle per beat (stroke volume) to the amount of blood within the left ventricle on the finish of diastole (end-diastolic volume), is broadly used clinically as an index of contractility. The ventricles comprise a continuum of muscle fibers originating from the fibrous skeleton on the base of the center (chiefly across the aortic orifice). They move towards the endocardium and progressively endure a 180-degree change in path to lie parallel to the epicardial fibers and to type the endocardium and papillary muscular tissues. At the apex of the heart, the fibers twist and switch inward to kind papillary muscles. Ventricular ejection can additionally be achieved by a decrease within the longitudinal axis as the center begins to slender towards the bottom. The early contraction of the apical part of the ventricles, coupled with the approximation of the ventricular walls, propels the blood towards the ventricular outflow tracts. Movement of the valve leaflets is basically passive, and the orientation of the cardiac valves is liable for the unidirectional flow of blood via the heart. The tricuspid valve, situated between the right atrium and the best ventricle, is made up of three cusps, whereas the mitral valve, which lies between the left atrium and the left ventricle, has two cusps. Attached to the free edges of these valves are fantastic, robust ligaments (chordae tendineae cordis) that come up from the highly effective papillary muscles of the respective ventricles. These ligaments forestall the valves from changing into everted throughout ventricular systole. In a normal heart, the valve leaflets remain relatively close together during ventricular filling. Anterior cusp Pulmonic valve Right cusp Left cusp Left cusp Aortic valve Right cusp Posterior cusp Anterior cusp Medial cusp Posterior cusp Anulus fibrosus Tricuspid valve Mitral valve Anterior cusp Posterior cusp Anulus fibrosus �. The pulmonic and aortic valves are located between the best ventricle and the pulmonary artery and between the left ventricle and the aorta, respectively. These valves consist of three cup-like cusps that are connected to the valve rings. At the end of the lowered ejection phase of ventricular systole, blood move Semilunar Valves briefly reverses towards the ventricles. This reversal of blood flow snaps the cusps collectively and prevents regurgitation of blood into the ventricles. In these sinuses, eddy currents develop, which tend to maintain the valve cusps away from the vessel partitions. Furthermore, the orifices of the best and left coronary arteries are behind the right and the left cusps, respectively, of the aortic valve. Were it not for the presence of the sinuses of Valsalva and the eddy currents developed therein, the coronary ostia could be blocked by the valve cusps, and coronary blood circulate would stop. The sac normally accommodates a small quantity of fluid, which offers lubrication for the continual movement of the enclosed coronary heart. Nevertheless, with the pericardium intact, a rise in diastolic pressure in one ventricle will increase the stress and decreases the compliance of the opposite ventricle. Heart Sounds Four sounds are usually generated by the guts, but only two are ordinarily audible via a stethoscope. With electronic amplification, the much less intense sounds can be detected and recorded graphically as a phonocardiogram. This means of registering faint coronary heart sounds helps delineate the exact timing of the guts sounds in relation to other occasions within the cardiac cycle. It is the loudest and longest of the center sounds, has a crescendo-decrescendo high quality, and is heard best over the Electrocardiogram apical area of the heart. The tricuspid valve sounds are heard finest in the fifth intercostal house just to the left of the sternum; the mitral sounds are heard best within the fifth intercostal space on the cardiac apex. The portion of the second sound caused by closure of the pulmonic valve is heard best in the second thoracic interspace just to the left of the sternum, whereas that attributable to closure of the aortic valve is heard best in the same intercostal area however to the best of the sternum. The aortic valve sound is mostly louder than the pulmonic valve, however in cases of pulmonary hypertension, the reverse is true. During expiration, a single heart sound is heard that reflects simultaneous closing of the pulmonic and aortic valves. However, during inspiration, closure of the pulmonic valve is delayed, mainly as a end result of elevated blood move from an inspiration-induced increase in venous return. A third coronary heart sound is sometimes heard in youngsters with skinny chest walls or in patients with left ventricular failure. It consists of some low-intensity, low-frequency vibrations heard greatest in the region of the cardiac apex. The vibrations happen in early diastole and are caused by the abrupt cessation of ventricular distention and by the deceleration of blood getting into the ventricles. It is caused by the oscillation of blood and cardiac chambers because of atrial contraction. This term is suitable because ventricular quantity remains fixed during this temporary interval. At the tip of ventricular ejection, a volume of blood approximately equal to that ejected during systole remains in the ventricular cavities. However, residual volume decreases somewhat when the guts price increases or when peripheral vascular resistance has diminished. Ventricular Diastole Isovolumic Relaxation into an earlier, shorter phase (rapid ejection) and a later, longer part (reduced ejection). The rapid ejection section is distinguished from the reduced ejection section by three characteristics: (1) a sharp rise in ventricular and aortic stress that terminates at peak ventricular and aortic pressure, (2) an abrupt decrease in ventricular volume, and (3) a pronounced improve in aortic blood move. The sharp lower in left atrial strain at the onset of ventricular ejection results from descent of the bottom of the heart and consequent stretching of the atria. During the reduced ejection interval, runoff of blood from the aorta to the peripheral blood vessels exceeds the speed of ventricular output, and aortic stress therefore declines. Throughout ventricular systole, the blood returning from the peripheral veins to the atria produces a progressive increase in atrial strain. During the fast ejection period, left ventricular strain barely exceeds aortic stress and aortic blood circulate accelerates (continues to increase), whereas during the decreased ventricular ejection section, aortic strain is larger and aortic blood circulate decelerates. This reversal of the ventricular-aortic stress gradient in the presence of steady circulate of blood from the left ventricle to the aorta is the end result of storage of potential energy within the stretched arterial walls. This saved potential power causes blood flow from the left ventricle into the aorta to decelerate. The peak of the move curve coincides with the purpose at which the left ventricular pressure curve intersects the aortic pressure curve during ejection.
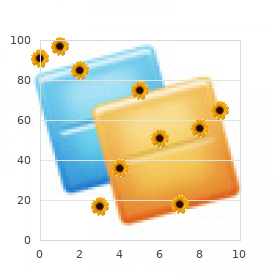
Purchase cheap lurantal lineFrom the bottom of the center, these fibers are distributed to the various chambers as an intensive epicardial plexus. In distinction to abrupt termination of the response after vagal activity, the consequences of sympathetic stimulation decay gradually after stimulation is stopped. Nerve terminals take as much as 70% of the norepinephrine launched throughout sympathetic stimulation; much of the rest is carried away by the bloodstream. Furthermore, the facilitatory results of sympathetic stimulation on the center attain steady-state values far more slowly than do the inhibitory results of vagal stimulation. The onset of the cardiac response to sympathetic stimulation begins slowly for two primary reasons. First, norepinephrine seems to be launched slowly from the sympathetic nerve terminals. The hypothalamic centers additionally provoke the cardiac response to alterations in environmental temperature. Experimentally induced temperature changes in the preoptic anterior hypothalamus alter the center fee and peripheral resistance. Stimulation of the parahypoglossal space of the medulla reciprocally prompts cardiac sympathetic pathways and inhibits cardiac parasympathetic pathways. In certain dorsal regions of the medulla, distinct cardiac accelerator sites (increase the center rate) and augmentor sites (increase cardiac contractility) have been detected in animals with transected vagus nerves. The accelerator areas are more plentiful on the proper aspect, whereas the augmentor websites are more prevalent on the left. Therefore, the sympathetic fibers mainly descend ipsilaterally through the brainstem. Baroreceptor Reflex Sudden modifications in arterial blood stress provoke a reflex that evokes an inverse change in heart rate. Baroreceptors situated in the aortic arch and carotid sinuses are liable for this reflex (see the part "Arterial Baroreceptors"). The inverse relationship between coronary heart price and arterial blood pressure is generally most pronounced over an intermediate vary of arterial blood pressures. Below this intermediate range, the heart rate maintains a continuing, excessive worth; above this pressure vary, the heart price maintains a continuing, low value. The results of modifications in carotid sinus strain on the exercise in cardiac autonomic nerves are described in. Below this vary of carotid sinus pressure, sympathetic activity is intense, and vagal activity is nearly absent. Conversely, above the intermediate vary of carotid sinus stress, vagal exercise is intense and sympathetic exercise is minimal. Control by Higher Centers Stimulation of varied brain regions can have significant effects on cardiac rate, rhythm, and contractility (see Chapter 11). In the cerebral cortex, centers that regulate cardiac operate are situated within the anterior half of the brain, principally within the frontal lobe, the orbital cortex, the motor and premotor cortex, the anterior portion of the temporal lobe, the insula, and the cingulate gyrus. Stimulation of the midline, ventral, and medial nuclei of the thalamus elicits tachycardia. Stimulation of the posterior and posterolateral areas of the hypothalamus can also change the center price. Stimuli utilized to the H2 area of Forel in the posterior hypothalamus evoke various cardiovascular responses, including tachycardia and associated limb movements; these adjustments resemble these observed during muscular exercise. Bainbridge reported that infusing blood or saline into canine accelerated their coronary heart fee. However, Bainbridge additionally noted that the center fee increased whenever central venous stress rose sufficiently to distend the right aspect of the center. When the center fee is slow, intravenous infusions of blood or electrolyte options normally speed up the center. Increases in blood quantity not only evoke Bainbridge reflex but also activate other reflexes (of note, the baroreceptor reflex). Therefore, modifications in coronary heart fee evoked by an alteration in blood quantity are the outcomes of these antagonistic reflex results. Evidently, the Bainbridge reflex predominates over the baroreceptor reflex when blood quantity rises, but the baroreceptor reflex prevails over the Bainbridge reflex when blood volume diminishes. Both atria have receptors that are affected by modifications in blood volume and that affect the heart fee. These receptors are located principally within the venoatrial junctions: in the best atrium at its junctions with the venae cavae and in the left atrium at its junctions with the pulmonary veins. Distention of these atrial receptors sends afferent impulses to the brainstem within the vagus nerves. The cardiac response to these modifications in autonomic neural exercise is highly selective. Even when the reflex enhance in heart fee is massive, modifications in ventricular contractility one hundred Vagal activity (% of max) Symp. Stimulation of the atrial receptors will increase not only the heart fee but also urine volume. Reduced activity within the renal sympathetic nerve fibers might partially account for this diuresis. However, the principal mechanism appears to be a neurally mediated reduction in vasopressin (antidiuretic hormone) secretion by the posterior pituitary gland (see Chapters 35 and 41). Respiratory Sinus Arrhythmia Rhythmic variations in coronary heart rate, occurring at the frequency of respiration, are detectable in most individuals and tend to be more pronounced in children. The coronary heart fee typically accelerates throughout inspiration and decelerates throughout expiration. Recordings from cardiac autonomic nerves reveal that neural activity will increase within the sympathetic fibers during inspiration and increases within the vagal fibers throughout expiration. This quick latency allows the heart fee to range rhythmically on the respiratory frequency. Conversely, the norepinephrine launched periodically on the sympathetic endings is removed very slowly. Thus respiratory sinus arrhythmia is brought about almost completely by modifications in vagal exercise. Stretch receptors within the lungs are stimulated throughout inspiration, and this action leads to a reflex increase in heart price. Intrathoracic pressure also decreases throughout inspiration and thereby will increase venous return to the proper aspect of the heart (see Chapter 19). After the time delay required for the elevated venous return to attain the left facet of the guts, left ventricular output will increase and raises arterial blood strain. This rise in blood strain in turn reduces the heart price by way of the baroreceptor reflex. The respiratory center within the medulla immediately influences the cardiac autonomic centers. In heart-lung bypass studies, the chest is opened, the lungs are collapsed, venous return is diverted to a pump-oxygenator, and arterial blood strain is maintained at a constant stage. In such studies, rhythmic motion of the rib cage attests to the exercise of the medullary respiratory facilities, and is commonly accompanied by rhythmic modifications in coronary heart rate on the respiratory frequency. This respiratory cardiac arrhythmia is kind of definitely induced by a direct interplay between the respiratory and cardiac centers in the medulla.
Cheap lurantal 20 mg without a prescriptionThis is named expiratory circulate limitation and could be demonstrated by asking a person to carry out three pressured expiratory maneuvers with growing effort. However, the circulate rates at decrease lung volumes converge; this means that with modest effort, maximal expiratory circulate is achieved. For this reason, expiratory circulate charges at lower lung volumes are said to be effort unbiased and circulate restricted as a outcome of maximal circulate is achieved with modest effort, and no amount of additional effort can improve the circulate rate beyond this restrict. In common the first 20% of the circulate within the expiratory flow-volume loop is effort dependent. Flow Limitation and the Equal Pressure Point Why is expiratory move restricted and reasonably effort independent Factors that restrict expiratory circulate are essential as a result of many lung ailments have an result on these factors and thus affect the quantity and velocity with which air is moved into and out of the lung. Flow limitation occurs when the airways, that are intrinsically floppy distensible tubes, turn out to be compressed. The airways become compressed when the pressure outdoors the airway exceeds the pressure inside the airway. The airways are proven as tapered tubes as a outcome of the total or collective airway crosssectional area decreases from the alveoli to the trachea. This constructive transpulmonary and transairway strain holds the alveoli and airways open. When an lively exhalation begins and the expiratory muscle tissue contract, pleural pressure rises to +60 cm H2O (in this example). Alveolar stress also rises, partly due to the rise in pleural pressure (+60 cm H2O) and partly because of the elastic recoil strain of the lung at that lung quantity (which on this case is 30 cm H2O). Because alveolar stress exceeds atmospheric strain, gasoline begins to flow from the alveolus to the mouth when the glottis opens. As gas flows out of the alveoli, the transmural pressure across the airways decreases. Thus as air strikes out of the lung, the driving stress for expiratory gasoline circulate decreases. In addition, the mechanical tethering that holds the airways open at high lung volumes diminishes as lung volume decreases. There is a point between the alveoli and the mouth at which the pressure inside the airways equals the pressure that surrounds the airways. Airways towards the mouth however nonetheless contained in the chest wall turn into compressed as a outcome of the strain outdoors is greater than the stress inside (dynamic airway compression). As a consequence the transairway strain now becomes unfavorable [Pta = Paw - Ppl = 58 - (+60) = -2 cm H2O] simply past the equal strain point. No quantity of effort will increase the circulate further because the upper pleural stress tends to collapse the airway at the equal strain level, just as it also tends to increase the gradient for expiratory gasoline move. It can be why airway resistance is greater throughout exhalation than throughout inspiration. In the absence of lung disease, the equal strain level happens in airways that contain cartilage, and thus they resist collapse. As lung volume decreases and as elastic recoil pressure decreases, the equal strain level strikes nearer to the alveoli. Dynamic Compliance One additional measurement of dynamic lung mechanics should be mentioned, and this is the measurement of dynamic compliance. Dynamic compliance is always less than static compliance, and it increases during train. This is because during tidal volume breathing, a small change in alveolar surface space is inadequate to deliver further surfactant molecules to the floor, and thus the lung is much less compliant. During exercise the other happens; there are giant adjustments in Inflation-deflation pressure-volume curve. Both of these respiratory actions are important for sustaining regular lung compliance. Changes within the mechanical properties of the lung or chest wall (or both) in the presence of illness result in an increase in the work of respiration. Respiratory muscle fatigue is the most common cause of respiratory failure, a course of by which gasoline change is insufficient to meet the metabolic wants of the body. In restrictive lung diseases, such as pulmonary fibrosis, lung compliance is decreased and the pressure-volume curve is shifted to the right. In obstructive lung illnesses, similar to asthma during an exacerbation or chronic bronchitis, airway resistance is elevated. With time or disease progression, these respiratory muscular tissues can fatigue and result in respiratory failure. The work of respiration is also elevated when deeper breaths are taken (an improve in tidal quantity requires more elastic work to overcome) and when the respiratory price increases (an improve in minute Ex p. Normal individuals and individuals with lung illness adopt respiratory patterns that minimize the work of breathing. For this purpose, individuals with pulmonary fibrosis (increased elastic work) breathe extra shallowly and quickly, and those with obstructive lung illness (normal elastic work but elevated resistive work) breathe more slowly and deeply. Individuals are inclined to adopt the respiratory fee at which the whole workofbreathingisminimal(arrow)forthosewithoutlungdisease. Airway resistance varies with the inverse of the fourth power of the radius and is larger in turbulent than in laminar move. Airway resistance decreases with increases in lung volume and with decreases in fuel density. Pulmonary perform checks (spirometry, flow-volume loop, body plethysmography) can detect abnormalities in lung operate earlier than individuals turn out to be symptomatic. Test results are in contrast with results obtained in normal individuals and range with sex, ethnicity, age, and top. Restrictive lung ailments are characterized by decreases in lung quantity, normal expiratory flow charges and resistance, and a marked lower in lung compliance. The equal strain point is the point at which the stress inside and surrounding the airway is the same. Specifically, as lung quantity and elastic recoil lower, the equal pressure level strikes towards the alveolus in normal people. Energy is expended during respiration to overcome the inherent mechanical properties of the lung. For people with elevated airway resistance, work is minimized by breathing at decrease frequencies. For people with restrictive lung ailments, work is minimized by shallow breathing at high frequencies. The dynamic compliance of the lung is at all times lower than the static compliance and will increase during exercise, sighing, and yawning. Define two kinds of dead house ventilation, and describe how lifeless area ventilation adjustments with tidal volume. Describe the composition of gasoline in ambient air, the trachea, and the alveolus, and understand how this composition adjustments with changes in oxygen fraction and barometric strain. Understand the alveolar carbon dioxide equation and identify how it modifications with alterations in alveolar ventilation. Compare the distribution of pulmonary blood circulate to the distribution of ventilation.
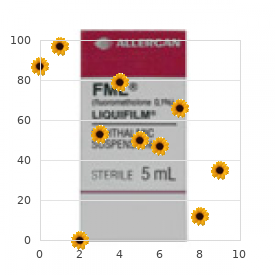
20mg lurantal with visaAs noted, at least three outward K+ currents (ito, iK, and iK1) contribute to the ultimate repolarization (phase 3) of the cardiac cell. These currents are subsequently essential determinants of the length of the plateau. For instance, the period of the plateau is substantially much less in atrial myocites than in ventricular myocytes. As Vm becomes increasingly negative during section three, the conductance of the channels that carry the iK1 present progressively increases and thereby accelerates repolarization. Similarly, many of the excess Ca++ ions that had entered the cell primarily throughout part 2 are eradicated principally by a 3Na+-Ca++ antiporter, which exchanges three Na+ ions for one Ca++ ion. As already famous, the length of the action potential in ventricular myocytes varies considerably with the location of these myocytes in the ventricular walls. In endocardial myocytes, by which the period of the motion potential is least, the magnitude of iK is biggest. The magnitude of iK and the period of the action potential are intermediate for epicardial myocytes. However, the iK1 channels contribute considerably to the speed of repolarization as quickly as section three has Slow-Response Action Potentials Fast-response motion potentials. The concentrations of tetrodotoxin had been 0mol/L intracingA,3�10-8 mol/LintracingB,3�10-7 mol/LintracingC, and3�10-6 mol/LintracingsDandE;EwasrecordedlaterthanD. In the management tracing (A), the everyday fast-response action potential displays a prominent notch, on account of ito, that separates the upstroke from the plateau. Progressively greater concentrations of tetrodotoxin produce a graded blockade of the quick sodium channels, as demonstrated in tracings B to E. In tracing E, the notch has disappeared, and the upstroke could be very gradual; this motion potential resembles a typical gradual response. In these cells, depolarization is achieved primarily by influx of Ca++ via L-type calcium channels as a substitute of influx of Na+ through quick sodium channels. Repolarization is completed in these fibers by inactivation of the calcium channels and by the elevated K+ conductance via the iK1 and iK channels. When the wave of depolarization reaches the end of the cell, the impulse is carried out to adjacent cells through hole junctions (see Chapter 2). Impulses cross more readily alongside the size of the cell (isotropic) than laterally from cell to cell (anisotropic) as a result of gap junctions are preferentially located on the ends of the cell. Gap junctions are rather nonselective in their permeability by ions and have a low electrical resistance that enables ionic current to move from one cell to another. The move of cost from cell to cell follows the principles of native circuit currents and therefore permits intercellular propagation of the impulse. Conduction of the Fast Response In fast- and slow-response fibers, the traits of conduction differ. In fast-response fibers, fast sodium channels are activated when the transmembrane potential of one region of the fiber suddenly changes from a resting value of roughly -90 mV to the brink value of approximately -65 mV. This portion of the fiber subsequently turns into a half of the depolarized zone, and the border is displaced accordingly. This process is repeated repeatedly, and the border strikes repeatedly down the fiber as a wave of depolarization. The conduction velocity alongside the fiber varies directly with the motion potential amplitude and the speed of change of the potential (dVm/dt) throughout section zero. The action potential amplitude is the potential distinction between the totally depolarized and the totally polarized regions of the cell interior. The magnitude of the native present is proportional to this potential distinction (see Chapter 5). The greater the potential distinction between the depolarized and polarized regions. The dVm/dt throughout phase 0 can be an necessary determinant of conduction velocity. If the lively portion of the fiber depolarizes progressively, the native currents between the resting area and the neighboring depolarizing area are small. The resting area adjacent to the active zone is depolarized steadily, and more time is subsequently required for each new section of the fiber to reach threshold. The resting membrane potential is another necessary determinant of conduction velocity. Changes within the resting membrane potential influence each the amplitude of the action potential and dVm/dt, which in flip alter the conduction velocity. Depolarization of Vm inactivates the quick sodium channels, which in flip decreases the amplitude of the motion potential and the dVm/dt, and as a consequence conduction velocity is slowed. The excitability traits of assorted types of cardiac cells differ considerably, relying on whether or not the motion potentials are quick or gradual responses. Fast Response Once the fast response has been initiated, the depolarized cell is now not excitable till it has partially repolarized. In the fast response, the interval from the beginning of the action potential until the fiber is prepared to conduct one other action potential is called the effective refractory interval which extends from the beginning of section 0 to a point in part 3 at which repolarization has reached approximately -50 mV. At approximately this value of Vm, most of the quick sodium channels have transitioned from the inactivated state to the closed state. When a quick response is evoked through the relative refractory period of a previous excitation, its characteristics vary with the membrane potential that exists on the time of stimulation. The later within the relative refractory interval that the fiber is stimulated, the greater are the will increase in the amplitude of the response and the slope of the upstroke because the variety of fast sodium channels that have recovered from inactivation will increase as repolarization proceeds. As a consequence, propagation velocity additionally will increase the later within the relative refractory period that the fiber is stimulated. This too displays the reality that when Vm is depolarized, more quick sodium channels are inactivated, and thus solely a fraction of the sodium channels are available to conduct the inward Na+ present throughout part zero. The threshold potential is approximately -40 mV for the slow response, and conduction is way slower than for the quick response. Also, fast-response fibers can reply at repetition charges that are a lot sooner than these of slow-response fibers. In this fiber, excitation very late in part 3 (or early in section 4) induces a small, nonpropagated (local) response (wave a). Still later in part 4, full excitability is regained, and theresponse(wavec)displaysnormalcharacteristics. Even after the cell has completely repolarized, it might be tough to evoke a propagated response for some time. This characteristic of slow-response fibers is called postrepolarization refractoriness. The amplitudes and upstroke slopes progressively improve as action potentials are elicited later within the relative refractory interval. Impulses that arrive early in the relative refractory period are performed much more slowly than those who arrive late in that interval. Even when gradual responses recur at low frequency, the fiber may be able to conduct solely a fraction of these impulses; for example, in certain circumstances, solely alternate impulses could also be propagated. Effects of Cycle Length Cycle size is the time between successive motion potentials. Changes in cycle size alter the period of the motion potential in cardiac cells.
Syndromes - Shallow breathing
- May appear as a nodule, papule, or macule and may look like hives
- Itching
- Surgery to correct the valve may be needed for children who continue to worsen or who have more serious complications
- Headache
- Unintentional weight loss
- Deficiency - Vitamin B9 (folacin)
- Nutritional (such as malnutrition)
- Rate of cell division or how quickly the tumor is growing
- Radioactive iodine
Cheap 5 mg lurantal overnight deliveryEleven of the 20 amino acids are synthesized within the body (nonessential amino acids), and the remaining nine amino acids are required in the food regimen (essential amino acids). Ten of the nonessential amino acids are derived from glucose by way of intermediates derived from glycolysis and the citric acid cycle. For instance, addition of an amino group from glutamate to the a-ketoacids pyruvate, oxaloacetate, and a-ketoglutarate produces alanine, aspartate, and glutamate, respectively. Cysteine receives its carbon skeleton from serine (product of 3-phosphoglycerate in glycolysis); however, its sulfur comes from the essential amino acid methionine. Removal of the a-amino group from amino acids is the preliminary step in the catabolism of amino acids. Nitrogen from the amino group is excreted as urea or incorporated into different compounds. Transamination entails the switch of the a-amino group of an a-amino acid to a-ketoglutarate, producing an a-keto acid from the amino acid and glutamate from a-ketoglutarate. Aminotransferases (transaminases) catalyze reversible transamination reactions that occur within the synthesis and the degradation of amino acids. Two mitochondrial reactions generate citrulline, which is transported to the cytosol. Ammonia is primarily transformed to urea, with the exception of ammonia derived from glutamine, which is used to acidify urine. Glutamate (1) Ammonia is derived from oxidative deamination of glutamate by glutamate dehydrogenase. Monoamines (1) Amine oxidases launch ammonia from epinephrine, serotonin, and histamine. Dietary protein (1) Bacterial ureases release ammonia from amino acids in dietary protein and from urea diffusing into the gut. Ammonia produced in extrahepatic tissues is poisonous and is transported in the circulation primarily as urea and glutamine. Signs and symptoms of hyperammonemia include feeding difficulties, vomiting, ataxia, lethargy, irritability, poor intellectual improvement, and coma. Glutamine carries ammonia in a nontoxic state; ammonia is launched in the kidneys for urine acidification. Transamination of amino acid nitrogen produces carbon skeletons of amino acids as a-keto acids that enter middleman metabolism at various points. Amino acids are categorized as glucogenic (degraded to pyruvate or intermediates in citric acid cycle), ketogenic (degraded to acetyl CoA or acetoacetyl CoA), or each glucogenic and ketogenic. Branched-chain amino acids-leucine, isoleucine, and valine-are degraded to branched-chain a-ketoacids that can enter the citric acid cycle. Methionine accepts a methyl group from methyl-folate to turn into S-adenosylmethionine, a common donor of a single carbon in metabolism. Succinyl CoA is formed from four amino acids by the use of propionyl CoA, which is a substrate for gluconeogenesis: isoleucine, valine, methionine, and threonine. Tyrosine is transformed by tyrosine hydroxylase into dopa, which is used to synthesize the catecholamines through a collection of intermediate reactions. Fumarylacetoacetate is transformed to fumarate, which is a substrate within the citric acid cycle, and acetoacetate. Branched-chain amino acids are metabolized primarily in muscle and to a lesser extent in different extrahepatic tissues. Branched-chain amino acid metabolism includes a collection of reactions ensuing in the conversion of leucine (ketogenic) into acetyl CoA and acetoacetate; isoleucine (ketogenic and glucogenic) into acetyl CoA and succinyl CoA; and valine (glucogenic) into succinyl CoA. Notice the position of methionine within the donation of methyl teams, resynthesis by homocysteine with the aid of vitamin B12 and folate, synthesis of cysteine, and production of succinyl CoA within the citric acid cycle. Methylated vitamin B12 (methyl-B12) transfers the methyl group to homocysteine, which produces methionine. Cystathionine, after an intermediate response, is converted to propionyl CoA and cysteine. Propionyl CoA can be produced by the metabolism of odd-chain fatty acids (see Chapter 7) and is an middleman product within the metabolism of the branched-chain amino acids valine and isoleucine. Deficiency of vitamin B12 results in an accumulation of methylmalonyl CoA and propionyl CoA, inflicting permanent neurologic dysfunction. Catecholamines (dopamine, epinephrine, and norepinephrine) are essential neurotransmitters which are derived from tyrosine and are formed by the dopa pathway in neural tissue and the adrenal medulla. Dopamine (primarily situated in the substantia nigra and ventral hypothalamus) is a neurotransmitter with multiple features that have an result on habits, particularly reward responses. Stimulation of the sympathetic nerves to the adrenal medulla causes the discharge of epinephrine and norepinephrine, which have an effect on blood vessels (vasoconstriction is larger with norepinephrine than epinephrine); the guts (contraction is larger with epinephrine than norepinephrine); and the gastrointestinal tract (both inhibit peristalsis). The reaction sequence for catecholamine synthesis begins with tyrosine, which is transformed to dopa by tyrosine hydroxylase (copper-containing rate-limiting enzyme) in the cytoplasm. Dopamine is converted to norepinephrine by dopamine hydroxylase, a coppercontaining enzyme, which uses ascorbic acid as a cofactor. N-Methyltransferase is positioned solely within the adrenal medulla; therefore, epinephrine is synthesized only in the adrenal medulla. Heme is crucial porphyrin and has a serious role in oxygen switch reactions. Heme is a cyclic planar molecule (like a wheel) with an iron atom on the center (hub) and an asymmetric arrangement of side chains around the rim. Step 3 (1) Porphobilinogen is transformed to hydroxymethylbilane by the cytosolic enzyme uroporphyrinogen I synthase (Table 8-3). Step 1 (1) Oxidases convert free heme to bilirubin in macrophages located within the spleen. The finish products of heme degradation are bilirubin and its degradative product, urobilinogen. Nitrogen Metabolism (2) Bilirubin diglucuronide, or conjugated (direct) bilirubin, is water soluble. Step four (1) Intestinal micro organism hydrolyze conjugated bilirubin and scale back free bilirubin to colorless urobilinogen. Viral hepatitis is associated with a combined hyperbilirubinemia (increase in unconjugated and conjugated bilirubin) as a outcome of problems with uptake, conjugation, and secretion of bilirubin into bile ducts. The first reaction within the metabolism of tryptophan is catalyzed by tryptophan hydroxylase, which converts tryptophan to 5-hydroxytryptophan. Serotonin (5-hydroxytryptamine) is synthesized primarily within the median raphe of the brainstem, pineal gland, and chromaffin cells of the intestine. Serotonin stimulates contraction of smooth muscle in the gastrointestinal tract, rising peristalsis, and it will increase the formation of blood clots when released from platelets as a vasoconstrictor of arterioles. The carcinoid syndrome, involving an oversecretion of serotonin, usually occurs when a carcinoid tumor of the small gut metastasizes to the liver. Serotonin produced by the metastatic nodules features access to the systemic circulation via hepatic vein tributaries and causes flushing of the pores and skin, sudden drops in blood stress, watery diarrhea. Coordinated activation or deactivation of key enzymes (usually by phosphorylation or dephosphorylation) b.
Cheap lurantal 30 mg amexThe primary capabilities of the stomach are storage and initiation of protein digestion. Regulation of gastric function is driven by extrinsic and intrinsic neural pathways together with key humoral (gastrin) and paracrine (histamine) mediators. The key secretions from the stomach are acid and pepsinogen, which together begin protein digestion. The abdomen additionally secretes intrinsic factor, which is involved in absorption of vitamin B12. The smooth muscle of the intestine wall undergoes cyclic modifications in membrane potential, termed the fundamental electrical rhythm or the gradual wave. The interstitial cells of Cajal are pacemakers in the gut wall, and so they set the frequency of the gradual wave. The proximal a half of the abdomen undergoes a gradual change in tone compatible with its storage function. The distal part of the stomach undergoes phasic contractions that can range considerably in strength. How are the varied parts of a blended meal digested and absorbed within the small gut What are the constituents and functions of pancreatic juice, and the way is their secretion controlled What are the mechanisms that provide for appropriate levels of fluidity of the intestinal contents What are the motor patterns of the small intestine in the postprandial period in addition to during fasting, and what functions do these patterns subserve The objective of this chapter is to discuss how such modifications are caused and how they end result finally in assimilation of nutrients. Changes in small intestinal perform that occur after the meal has handed via may also be addressed. The small intestine is the critical portion of the intestinal tract for assimilation of nutrients. In this website the meal is blended with a selection of secretions that allow its digestion and absorption, and motility features guarantee adequate mixing and publicity of the intestinal contents (chyme) to the absorptive surface. The small intestine has many specializations that allow it to carry out its features effectively. One of the most obvious specializations is the substantial surface space of the mucosa; that is achieved in a variety of other ways. The primary attribute of the small intestinal section of the response to a meal is managed supply of chyme from the abdomen to match the digestive and absorptive capacity of the intestine. Therefore the function of this region is very regulated by suggestions mechanisms that involve hormonal, paracrine, and neural pathways. The stimuli that regulate these processes are both mechanical and chemical and embody distention of the intestinal Gastric Emptying in the Small Intestinal Phase Immediately after a meal the abdomen could comprise up to a liter of material that may empty slowly into the small intestine. The price of gastric emptying depends on the macronutrient content material of the meal and the quantity of solids it incorporates. Thus solids and liquids of comparable nutritional composition will empty at different rates. Regulation of gastric emptying is achieved by alterations in motility of the proximal a part of the abdomen (fundus and corpus) and distal a part of the stomach (antrum and pylorus) as properly as within the duodenum. Recall that during the esophageal and gastric part of the meal, the predominant reflex response is receptive relaxation. At the same time, peristaltic movements within the more distal part of the abdomen (antrum) mix the gastric contents with gastric secretions. This same pathway is responsible for the inhibition of gastric acid secretion that happens when vitamins are within the duodenal lumen. This hormone is physiologically necessary, along with its position in neural pathways, in the regulation of gastric emptying, gallbladder contraction, relaxation of the sphincter of Oddi, and pancreatic secretion. At this time, intragastric stress in the proximal portion of the stomach will increase, thereby shifting materials into the antrum and toward the antral pump. Antral peristaltic contractions once more deepen and culminate in opening of the pylorus and launch of gastric contents into the duodenum. Liquids and the semiliquid chyme circulate down the pressure gradient from the stomach to the duodenum. As the meal enters the small gut, it feeds again through both neural and hormonal pathways to regulate the rate of gastric emptying based on the chemical and physical composition of the chyme. Afferent neurons, predominantly of vagal origin, respond to nutrients, [H+], and the hyperosmotic content material of chyme as it enters the duodenum. Reflex activation of vagal efferent outflow decreases the power of antral contractions, contracts the pylorus, and reduces proximal gastric motility (with a decrease in intragastric Pancreatic Secretion Most of the nutrients ingested by people are within the chemical type of macromolecules. However, such molecules are too giant to be assimilated throughout the epithelial cells that line the intestinal tract and should therefore be broken down into their smaller constituents by processes of chemical and enzymatic digestion. Secretions arising from the pancreas are quantitatively the most important contributors to enzymatic digestion of the meal. The pancreas additionally offers additional necessary secretory products that are very important for normal digestive perform. The latter are involved in neutralizing gastric acid in order that the small intestinal lumen has a pH approaching 7. This is important as a result of pancreatic enzymes are inactivated by high levels of acidity and also as a end result of neutralization of gastric acid reduces the chance that the small intestinal mucosa might be injured by such acid appearing in combination with pepsin. Quantitatively the pancreas is the most important contributor to the provision of bicarbonate ions wanted to neutralize the gastric acid load, though the biliary ductules and duodenal epithelial cells additionally contribute. As in the salivary glands, the pancreas has a construction that consists of ducts and acini. The pancreatic acinar cells line the blind ends of a branching ductular system that finally empties into the main pancreatic duct and from there into the small intestine beneath management of the sphincter of Oddi. Also in widespread with salivary glands, a primary secretion arises within the acini, which is subsequently modified as it passes by way of the pancreatic ducts. In common the acinar cells supply the organic constituents of the pancreatic juice in a main secretion whose ionic composition is corresponding to that of plasma, whereas the ducts dilute and alkalinize the pancreatic juice while reabsorbing chloride ions. Many of the digestive enzymes produced by the pancreas, notably the proteolytic enzymes, are produced as inactive precursor types. Storage in these inactive forms is critically important in preventing the pancreas from digesting itself. The ducts of the pancreas can be thought of the effector arm of a pH regulatory system designed to respond to luminal acid in the small intestine and secrete simply sufficient bicarbonate to restore pH to neutrality. This regulatory function additionally requires mechanisms to sense luminal pH and convey this info to the pancreas in addition to different epithelia. The pH-sensing mechanism is embodied in specialized endocrine cells often known as S cells, localized inside the small intestinal epithelium. Thus as secretin evokes secretion of bicarbonate, pH in the small intestinal lumen will rise and the signal for launch of secretin from S cells will be terminated. At the mobile level, secretin stimulates epithelial cells to secrete bicarbonate into the ductular lumen, with water following through the paracellular route to maintain osmotic equilibrium. This secondarily drives the activity of an adjoining antiporter that exchanges the chloride ions for bicarbonate. Some is taken up across the basolateral membrane of the ductular epithelial cells Lipid-Digesting Enzymes or Precursors Lipase Nonspecificesterase ProphospholipaseA2 pH in duodenum Ductular bicarbonate secretion Nucleases Deoxyribonuclease Ribonuclease Regulatory Factors Procolipase Trypsininhibitors Monitorpeptide S cells Secretin release �.
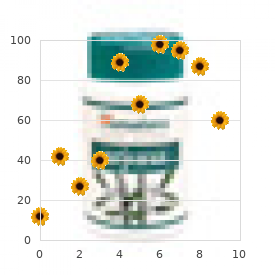
Order lurantal 30mg with visaIn cardiac muscle, the rise in intracellular [Ca++] could be regulated, which affords the guts an important technique of modulating the drive of contraction with out recruiting more muscle cells or undergoing tetany. Moreover, tetany of cardiac muscle cells would forestall any pumping motion and thus be deadly. Consequently, the center relies on completely different means of accelerating the drive of contraction, together with varying the amplitude of the intracellular Ca++ transient. In particular, some Ca++ is extruded from the cardiac muscle cell though the sarcolemmal 3Na+-Ca++ antiporter and a sarcolemmal Ca++ pump. Similarly, [Na+] is considerably greater within the extracellular media than inside the cell. The antiporter makes use of the Na+ gradient throughout the cell to power the uphill movement of Ca++ out of the cell. Because three Na+ ions enter the cell in exchange for one Ca++ ion, the 3Na+-Ca++ antiporter is electrogenic and creates a depolarizing current. Although the interplay of actin and myosin requires a relatively small increase in free intracellular [Ca++], the abundance of Ca++-binding proteins within the myoplasm necessitates a a lot larger improve in total intracellular [Ca++]. The resting intracellular [Ca++] is approximately 50 to one hundred nmol/L; half-maximal pressure of contraction requires roughly 600 nmol/L of free Ca++. However, due to Ca++-binding proteins corresponding to parvalbumin and troponin C, the total myoplasmic concentration should enhance by 70 �mol/L. Thus as much as 30% of the rise in intracellular [Ca++] may be attributable to influx of Ca++ via voltage-gated calcium channels within the sarcolemma, and the 3Na+-Ca++ antiporter contributes considerably to Ca++ extrusion during leisure. The sarcolemmal Ca++ pump is in lower abundance than the 3Na+-Ca++ antiporter however has a better affinity for Ca++ and thus may contribute more to the regulation of resting intracellular [Ca++]. The relative contribution of the Ca++ extrusion mechanisms, however, varies between species. A easy technique of modulating the pressure of contraction of cardiac muscle cells in vitro is to range extracellular [Ca++]. In vivo, a rise in the measurement of the intracellular Ca++ transient and hence the drive of contraction occurs in response to sympathetic stimulation (see the part "-Adrenergic Agonists" and in addition Chapter 18). Sympathetic stimulation often occurs in periods of excitement or fright and involves activation of -adrenergic receptors on the guts by norepinephrine (released from nerve terminals in the heart) or epinephrine (released from the adrenal medulla into the bloodstream). Typically, the speed of leisure accompanying this -adrenergic stimulation also increases, which results in a shorter contraction. The frequency of contractions of the guts additionally increases with -adrenergic stimulation and is termed constructive chronotropy. Thus -adrenergic stimulation of the center produces stronger, briefer, and extra frequent contractions. Moreover, tetany of the center can be lethal because it would defeat the important pumping action of the guts. The coronary heart has due to this fact developed various strategies to increase the drive of contraction. The lengthy duration of the action potential found in cardiac muscle, which is due to activation of the voltage-gated L-type calcium channel, ends in a protracted refractory interval, which in flip prevents tetany. Isoproterenol (a -adrenergic receptor agonist) increases the amplitudeoftheintracellularCa++transientandhencetheamountof forcegenerated(B). An extra consequence of sympathetic stimulation is an increase in heart price through a direct effect on the pacemaker cells (see Chapter 18). In contrast, skeletal muscle typically displays maximal rigidity at resting length. Stretching of the heart in vivo happens during instances of elevated venous return of blood to the center. The significance of this mechanism is that it helps the heart pump whatever quantity of blood it receives. Thus when the heart receives a lot of blood, the ventricles are stretched, and the force of contraction is increased, which ensures ejection of this extra volume of blood. Stretching of cardiac muscle also increases passive rigidity, which helps stop overstretching of the center. This passive resistance within the heart is greater than that in skeletal muscle and is attributed to each extracellular matrix (connective tissue) and intracellular elastic proteins (titin). This stretch-induced improve in pressure of contraction of cardiac muscle occurs over a slim vary of sarcomere lengths (ca. This ascending limb of the length-tension relationship in cardiac muscle is way steeper than that seen in skeletal muscle. It is necessary to note that this stretch-induced increase in pressure can occur inside a singe heart beat. The mechanism(s) underlying this stretch-induced enhance in drive of contraction of cardiac muscle is controversial, however appears to contain modifications within the overlap of the thick and thin filaments as nicely as stretch-induced improve in the Ca++ sensitivity of contraction. In rat ventricular trabecular muscle, approximately 60% of the stretch-induced improve in force of contraction has been attributed to an increase in Ca++ sensitivity, whereas the remaining 40% of the stretch-induced improve in drive of contraction has been attributed to modifications in the overlap of the thick and thin filaments. The modifications in myofilament overlap, however, are much less prone to contribute to the continued improve in drive of cardiac contraction as sarcomere length will increase from 2. RyR Sarcoplasm Cardiac Muscle Hypertrophy Exercise corresponding to endurance operating can improve the dimensions of the center because of hypertrophy of individual cardiac muscle cells. In distinction, if exposed to chronic pressure overload, the guts might bear both concentric left ventricular hypertrophy or dilated left ventricular hypertrophy, which causes impairment of operate. Details regarding the morphological, useful, and mechanistic variations between these numerous kinds of hypertrophy may be discovered elsewhere on this textbook (see Chapter 18). Concentric hypertrophy is characterised by thickening of the left ventricular wall and represents a compensatory hypertrophy to the increased load. Dilated hypertrophy is characterised by increased ventricular volume (end-diastolic volume). Both concentric/compensatory left ventricular hypertrophy and dilated left ventricular hypertrophy have been shown to exhibit decreased contractile response to -adrenergic stimulation, which limits the contractile reserve. It also appeared to inhibit maladaptive transforming of the guts after ischemia/ reperfusion harm. The hyperlink or hyperlinks between cardiac hypertrophy, decreased cardiac performance, and impaired -adrenergic response during persistent stress overload are unclear. Decreased cardiac efficiency has been attributed to dysregulation of intracellular [Ca++]. There is proof that cardiac hypertrophy is in all probability not related to some functional impairments. Cardiac muscle cells are comparatively small (10 �m � 100 �m) and type an electrical syncytium with tight electrical and mechanical connections between adjacent cardiac muscle cells. Action potentials are initiated within the sinoatrial node and spread rapidly throughout the heart to permit synchronous contraction, a function essential for the pumping action of the heart. Contraction of cardiac muscle includes the Ca++dependent interplay of actin and myosin filaments, as in skeletal muscle. However, unlike skeletal muscle, cardiac muscle requires an inflow of extracellular Ca++.
Discount lurantal american expressIn the small gut, retinol is converted to retinol esters, the key storage form of vitamin A. Sources of vitamin D embody liver, egg yolk, saltwater fish, and vitamin D�fortified meals. Preformed vitamin D in the food plan consists of cholecalciferol (vitamin D3) and ergocalciferol (vitamin D2, present in plants), which is interconvertible with vitamin D3. Endogenous vitamin D is produced by photoconversion of 7-dehydrocholesterol to vitamin D3 in sun-exposed pores and skin (most essential supply of vitamin D). Inadequate publicity to daylight: decreased synthesis of cholecalciferol (vitamin D3) b. Vitamin E deficiency is uncommon and primarily occurs in kids with malabsorption attributable to cystic fibrosis and in abetalipoproteinemia (see Chapter 7). Sources of vitamin K embrace green leafy vegetables (which supply vitamin K1, phylloquinone) and bacterial synthesis within the colon (which supplies vitamin K2, or menaquinone). When g-carboxylated in the liver by vitamin K and launched into the circulation, these coagulation components are in a place to bind to calcium, which is crucial to the formation of a fibrin clot. Therapy with coumarin (warfarin) derivatives: inhibits hepatic epoxide reductase b. Newborns: lack bacterial colonization of the bowel and should obtain an intramuscular vitamin K injection at delivery to forestall hemorrhagic illness of the newborn 6. Clinical findings related to vitamin K deficiency and extra (see Table 4-2) V. Calcitonin, which is synthesized by C cells within the thyroid gland, inhibits osteoclasts, thereby inhibiting the release of calcium from bones. Coumarin derivatives are present in rat poison, which is a standard explanation for poisoning in kids. Muscle contraction: modulates the vasoconstrictive effects of intracellular calcium d. Osmotic diuresis: most typical cause; loss of a hypotonic salt answer within the kidneys because of glucosuria, extra urea, or mannitol. Diabetes insipidus: lack of water as a end result of deficiency or dysfunction of antidiuretic hormone 6. Clinical findings related to hyponatremia and hypernatremia (see Table 4-3) E. Regulates insulin secretion: hypokalemia inhibits insulin; hyperkalemia stimulates insulin secretion 3. Arterial pH (1) Alkalotic conditions cause hydrogen ions to transfer out of the cell (provides protons) and potassium to move into the cell (leads to hypokalemia) to preserve electroneutrality. Respiratory and metabolic alkalosis: most typical cause; alkalosis enhances glycolysis and phosphorylation of glucose b. Hypovitaminosis D as a result of malabsorption: decreased intestinal absorption of phosphate c. Clinical findings associated with hypophosphatemia and hyperphosphatemia (see Table 4-3) G. Aldosterone: controls renal reabsorption (when present) and excretion (when absent) 4. In renal tubular acidosis and diarrhea, the loss of bicarbonate causes a rise in chloride ranges to offset the loss of unfavorable expenses. Iron capabilities in oxygen transport, the electron transport chain, and as an enzyme cofactor; deficiency symptoms are anemia, Plummer-Vinson syndrome, and fatigue. Iodine functions within the synthesis of thyroid hormones; deficiency produces goiter. Chromium is a element of the glucose tolerance factor; deficiency produces impaired glucose tolerance. Fluoride capabilities in the structure of hydroxyapatite; deficiency produces dental caries. Iron is the structural part of heme in hemoglobin, myoglobin, and the cytochrome oxidase system. Meat contains heme iron, which is ferrous (Fe2�) and out there for absorption within the duodenum. Iron poisoning (1) Common in kids (2) Causes hemorrhagic gastritis and liver necrosis b. Alkaline phosphatase (1) Important in bone mineralization (2) Marker of obstruction to bile flow in the liver or frequent bile duct 3. It is secreted into the plasma, where it represents 90% to 95% of the entire serum copper focus. Iodine deficiency is due primarily to an insufficient consumption of seafood or iodized table salt. An excess in fluoride primarily outcomes from an extra of fluoride in ingesting water. Redox coenzymes serve as provider molecules for hydrogen and electrons during biologic oxidation-reduction reactions B. The amount of lower in free vitality in kcal/mole is the quantity of free vitality a response will release or require. Hydrolysis of other nucleoside triphosphates and different high-energy compounds supplies energy for quite lots of metabolic processes. Inner membrane: oxidative phosphorylation Acetyl CoA: product of fat and glucose oxidation Acetyl CoA: a focus in metabolism fifty six Rapid Review Biochemistry energy-yielding main nutrients. Glycolysis, glycogenesis, glycogenolysis, pentose phosphate shunt, fatty acid synthesis, steroid synthesis. Each reaction in a pathway has distinctive traits relating to substrates, products, enzymes, cofactors, and inhibitors. At least one step in a metabolic pathway is usually regulated by hormones or metabolites that limit or speed up the circulate of metabolites through the pathway. Significant reduction within the exercise of an enzyme catalyzing one step in a pathway, attributable to a genetic defect or inhibitor, leads to accumulation of some metabolites and reduced ranges of others, typically with pathologic penalties. Generation of Energy from Dietary Fuels 5-5: Schematic diagram of a mitochondrion reveals the situation of key enzymes. Condensation of acetyl CoA with oxaloacetate to form 6-carbon citrate begins the cycle. Replenishing reactions restore cycle intermediates which may be drained off to biosynthetic pathways or wanted in higher quantities. Various amino acids are converted to acetyl CoA, a-ketoglutarate, succinyl CoA, fumarate, or oxaloacetate. Carbons from glucogenic amino acids and pyruvate enter the cycle as intermediates which are convertible to malate, which is exported to the cytosol and converted to oxaloacetate to enter the gluconeogenic pathway (see Chapter 6). Coenzyme Q (CoQ) and cytochrome c, two smaller carriers, shuttle electrons between the large complexes.
Cheap 5 mg lurantal visaOne mechanism for such an impact entails the release of corticotropin-releasing issue from the hypothalamus. It has sensory and motor components, and the motor component consists of sympathetic and parasympathetic divisions. The enteric nervous system is usually thought-about as part of the autonomic nervous system however is anxious specifically with management of the gastrointestinal tract. Sympathetic preganglionic neurons are positioned in the thoracolumbar area of the spinal twine, and sympathetic postganglionic neurons are situated in paravertebral and prevertebral ganglia. Parasympathetic preganglionic neurons are situated in cranial nerve nuclei or within the sacral portion of the spinal cord. Parasympathetic postganglionic neurons reside in ganglia positioned in or near the target organs. Most function to activate reflexes; for some, activation additionally leads to sensations that are experienced consciously. The enteric nervous system consists of the myenteric and submucosal plexuses in the wall of the gastrointestinal tract. The myenteric plexus regulates motility, and the submucosal plexus regulates ion and water transport and secretion. Neurotransmitters at the synapses of preganglionic neurons in autonomic ganglia include acetylcholine (acting at both nicotinic and muscarinic receptors) and a quantity of neuropeptides. Norepinephrine (acting on adrenergic receptors) is the neurotransmitter usually released by sympathetic postganglionic neurons; neuropeptides are additionally launched. Sympathetic postganglionic neurons that offer sweat glands release acetylcholine. Parasympathetic postganglionic neurons launch acetylcholine (acting on muscarinic receptors). The pupil is controlled reciprocally by the sympathetic and parasympathetic nervous techniques. Sympathetic exercise causes pupillary dilation (mydriasis); parasympathetic exercise causes pupillary constriction (meiosis). Emptying of the urinary bladder depends on parasympathetic outflow in the course of the micturition reflex. Sympathetic constriction of the interior sphincter of the urethra prevents voiding. The hypothalamus incorporates many nuclei that have a wide selection of functions related to regulation of primary bodily capabilities, including body temperature, body weight, and fluid consumption. The goal of hypothalamic function is to maintain homeostasis of crucial physiological parameters by performing as a servomechanism. The hypothalamus receives details about specific physiological parameters and makes use of this info to keep each of these parameters at a specific set level. This chapter illustrates the method it maintains homeostasis by way of its control of the autonomic system. Describe the organization of skeletal muscle, including the structural features/proteins throughout the skeletal muscle fiber that link the contractile components to the extracellular matrix and bone to effect movement. While describing the varied linkages, identify congenital conditions that generally affect particular constructions and how they could contribute to a myopathy. Describe the molecular mechanisms by which an motion potential within the motor neuron in the ventral horn of the spinal column can lead to contraction of a skeletal muscle. Describe the mechanisms by which the drive of skeletal muscle contraction increases. Compare skeletal muscle fiber sorts in phrases of recruitment sample, metabolic characteristics, contractile traits, and thus their suitability for various kinds of activity. Discuss the signaling pathways that contribute to the expression of the slow-twitch muscle phenotype versus the fast-twitch muscle phenotype. Discuss the length-tension curves and force-velocity curves for skeletal muscle, including the molecular bases of both curves. When considered underneath the microscope, skeletal muscle exhibits transverse striations (at intervals of 2 to three �m) that outcome from the extremely organized arrangement of actin and myosin molecules within the skeletal muscle cells. Smooth muscle (which lacks the striations evident in skeletal and cardiac muscle) is an involuntary muscle sometimes found lining hollow organs such as the gut and blood vessels. In all three muscle varieties, force is generated by the interplay of actin and myosin molecules, a course of that requires transient elevation of intracellular [Ca++]. In this chapter, consideration is directed on the molecular mechanisms underlying contraction of skeletal muscle. To put this information into perspective, you will need to first look at the fundamental group of skeletal muscle. The point of attachment closest to the backbone (proximal) is recognized as the origin, whereas the purpose of attachment on the far facet of the joint (distal) is called the insertion. These factors of attachment happen via tendons (connective tissue) at the end of the muscle. Note that the point of insertion is near the elbow joint, which enables a broad vary of movement. Also notice that the joint is spanned by a flexor muscle on one aspect and an extensor muscle on the opposite aspect of the joint. Each muscle consists of quite a few cells called Skeletal Muscle Physiology Muscle cells are highly specialised for the conversion of chemical power to mechanical vitality. Because work can take many varieties (such as locomotion, pumping blood, or peristalsis), several forms of muscle have developed. The three basic kinds of muscle are skeletal muscle, cardiac muscle, and easy muscle. Skeletal Muscle Attaches to the Skeleton by Way of Tendons and Typically Spans a Joint. The proximal and distal factors of attachment of the tendon are termed origin and insertion, respectively. Individual muscle fibers are then grouped together into fascicles, which are surrounded by another connective tissue layer known as the perimysium. Within the perimysium are the blood vessels and nerves that offer the individual muscle fibers. At the ends of the muscle, the connective tissue layers come collectively to kind a tendon, which attaches the muscle to the skeleton. The myotendinous junction is a specialized area of the tendon the place the ends of the muscle fibers interdigitate with the tendon for the transmission of the force of contraction of the muscle to the tendon to effect motion of the skeleton (discussed later in this section). The tendon and the connective tissue layers are composed primarily of elastin and collagen fibers, and thus they also contribute to passive tension of muscle and forestall harm to the muscle fibers because of overstretching or contraction. Individual skeletal muscle cells are narrow (10 to 80 �m in diameter), however they can be extraordinarily lengthy (up to 25 cm in length). Each skeletal muscle fiber accommodates bundles of filaments, referred to as myofibrils, working alongside the axis of the cell.
References - Triano, J. J. (2001). Biomechanics of spinal manipulative therapy. Spine Journal, 1(2), 121n130.
- Hofer DR, Sherwood ER, Bromberg WD, et al: Autonomous growth of androgen independent human prostatic carcinoma cells: role of transforming growth factor-?, Cancer Res 51:2780n2785, 1995.
- Pico JL, Rosti G, Kramar A, et al: A randomised trial of high-dose chemotherapy in the salvage treatment of patients failing first-line platinum chemotherapy for advanced germ cell tumours, Ann Oncol 16:1152n1159, 2005.
- Miller KS, McAninch JW: Radiographic assessment of renal trauma: our 15-year experience, J Urol 154:352n355, 1995.
- Ryall RL, Grover PK, Stapleton AM, et al: The urinary F1 activation peptide of human prothrombin is a potent inhibitor of calcium oxalate crystallization in undiluted human urine in vitro, Clin Sci 89:533n541, 1995.
|
|