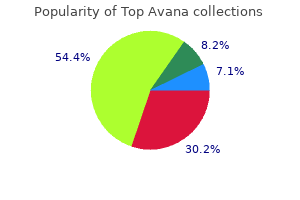
Professor, Department of Anesthesiology and Critical Care Medicine
Professor, Department of Biomedical Engineering
Johns Hopkins Medicine
Baltimore, Maryland
This could be differentiated from venous hum in following manner: Venous hum: Heard decrease within the neck, suppressed by compression of ipsilateral neck vein statistics of erectile dysfunction in us buy generic top avana on-line. Transmitted impulses type aortic stenosis and aortic sclerosis Can be differentiated by associated cardiac examination jack3d causes erectile dysfunction top avana 80 mg low price. Most frequent form of goiter: z Euthyroid: Multinodular goiter Hashimoto thyroiditis erectile dysfunction diabetes medication cheap top avana uk. Differentiation of Goiter from Normal Gland Normally thyroid gland barely visible and barely palpable as a outcome of interference of assorted surrounding buildings, sternocleidomastoid muscle tissue erectile dysfunction treatment cincinnati buy discount top avana 80mg on-line. Anterior neck plenty: this can be differentiated by asking the affected person to swallow: Branchial cyst Cervical lymphadenopathy Pharyngeal diverticula erectile dysfunction pump australia top avana 80 mg line. Detection of goiter in extended neck is less reliable than detection and palpation of goiter in normal neck position, which is more dependable erectile dysfunction talk your doctor order top avana paypal. Skin: Warm and moist skin Pretibial myxedema Palmar erythema Hyperpigmentation at pressure points Onycholysis Friable nail. Findings suggestive of hyperthyroidism z Lid lag z Lid retraction z Fine tremor z Worm and moist pores and skin z Tachycardia. Pretibial Myxedema Localized nonpitting edema, well demarcated, raised, bilateral pinkish/brownish nodules on the anterior side of shin. Thyroid Gland 1293 Thyroid acropathy that is characterised by: z Clubbing z Subperiosteal deposition of bones in palms and toes not in lengthy bones-painless and asymptomatic. Proptosis could be precisely measured by: Hertel exophthalmometer handheld system to measure that distance between lateral orbital rim and anterior corneal floor. Onycholysis Partial separation of distal and lateral attachments of nail plate kind nailbed is called onycholysis. Outer a part of shaft composed of compact bone-covered by a connective tissue sheath-periosteum. Long bones found in limbs-humerus, tibia, fibula, radius, ulna, femur, metacarpals and metatarsals. These are composed of thin layer of compact bone, inside is made up of cancellous bone. Sesamoid Bones these are small nodular bones found in sure tendons, the place they rub over bony surfaces. Largest sesamoid bone in patella, over the tendon of flexor pollicis brevis, and flexor hallucis brevis. Cartilage It is a connective tissue sheath in which cells and fibers are embedded in gel like matrix. Cartilage is roofed by fibrous membrane known as perichondrium, except on uncovered surfaces in joints. It is discovered in the disc throughout the joints (temporomandibular joint, sternoclavicular joint, knee joint) and on articular surfaces of the clavicle and mandible. Elastic Cartilage Large variety of elastic fibers embedded in small quantity of matrix. Joints this can be defined by an area the place two or extra bones come along with or with none movement. Examples: Union between epiphysis and diaphysis of lengthy bones Union between manubrium sterni and 1st rib. Joint cavity is lined by a synovial membrane extending from margin of one articular surface to other. In some joints (knee joint) a wedge-shaped fibrocartilage is current between two articular floor known as articular disc. The ligaments are normally present outside the capsule however few ligaments like cruciate ligaments lie throughout the capsule. Movements: Flexion, extension, abduction, adduction, medial rotation, lateral rotation, and circumduction. Fibrous kind of ligament: It prevents excessive movement in a joint but in severe stress-this ligament can be stretched. Elastic ligament: this kind of ligament is stretchable and could be reverted again to regular size. Outer layer of dense concentric bundles of collagen, the annulus fibrosus encloses a core of hydrated tissue-nucleus pulposus. Muscles Muscle fibers are divided into two sorts according to their pace of motion: 1. Slow twitch muscle fiber � � � � � � � � � Innervated by slowly conducting nerve fiber Have low threshold Conduct slowly Recruitment begins with sluggish unit Firing frequency ranges from 10�20 Hz High myoglobin content Use oxidative mechanism for vitality formation Fatigue resistant It produce sustained muscle contraction Fast twitch muscle fiber � � � � � � � � � Innervated by rapidly conductions nerve fiber Have high threshold Conduct rapidly Recruitment later progresses to larger items Firing frequency ranges from one hundred Hz Low myoglobin content Use glycolysis for power formation Fatigable It produces sudden muscle contraction, quick lived Symptoms Related to Bone Pain Deep boring, localized (in case of trauma, tumor, infection) or generalized (osteoporosis), sharp piercing (fracture). Symptoms Related to Joint Pain Site of ache: Irritation of construction close to pores and skin produces nicely localized ache. Pain in deeper constructions produces poorly localized ache, segmental in distribution known as sclerotomal distribution, it differs from particular dermatomal distribution. Radiation of ache: Deeper pain could also be felt at some extent far from deeper structure. Disorder of lower lumbar spine could also be referred to upper lumbar back ache because posterior longitudinal ligament is innervated by higher lumbar nerves. Severity of pains: Acute onset-Gouty arthritis, infective arthritis Waxing and waning-Rheumatoid arthritis Progressively improve in pain-infective origin. Aggravating and relieving elements: Improving with exercise, returning at rest-inflammatory joint disease. Pain steadily worsen through the course of days- mechanical joint illness (osteoarthritis). Regarding Crepitations It is a grating sensation on palpation on the joint site-it might fantastic or coarse, it might be audible or palpable. Locking Locking occurs when foreign materials shall be accumulated in between two articular surfaces. Symptoms Related to Muscles Pain Pain and stiffness: Deep, fixed, poorly localizing ache. Whether weak spot is fluctuating-it weak spot worsens through the course of activity-myasthenia gravis. If Whether weak point is sudden or gradual and progressive: 1312 Clinical Methods and Interpretation in Medicine � Sudden entrapment of peripheral nerve (traumatic radial nerve palsy)-it will enhance with time � If the weak spot in progressive-Motor neuron disease. Questions to be requested in case of muscle weakness: Whether the weak point is global or focal Wasting and fasciculation: this might be seen during history taking as muscle twitching in numerous muscular tissues or single muscular tissues or calf. Cramp: It might happen in any muscle mainly in calf muscle-it could be triggered by forceful contraction of muscle. Following rules to be followed throughout musculoskeletal examinations are: Examination of bone: Look for limb shortening Any local tenderness. Examination of joints: Inspection: Swelling: Causes could additionally be: � Effusions � Thickening of synovial tissue � Thickening of bony margins. Watch that thickening is especially due to joint swelling or swelling of adjacent construction. Skin changes-Watch: � Color of pores and skin � Temperature � Redness � Tension around the joint. Tenderness: Tenderness to be elicitated in: � Joint margin � Adjacent bony surfaces � Surrounding ligaments and tendons. Temperature: It could be measured in following manners: � For small joint: For example, metacarpophalangeal, interphalangeal joints measure the temperature with fingertips of the examiner and compare with comparable joints of different arms. To look at the range of motion, begin with joint within the impartial position: � Lower limb extended with ft dorsiflexed to 90�. Assess the lively movement of the backbone and passive movements of the limb joints-its energetic movement is restricted; it is as a result of of muscle weak point. From impartial place, measure the diploma of extension or flexion: � In few joints, usually no extension happen. In knee joint, movement of the knee may be described as hyperextension of knee joint. Arms: From in entrance, ask the affected person to place his both hand on the back of the top, and elbows again. Squeeze the small joints (metatarsophalangeal and interphalangeal joints) to elicit tenderness, any deformity, any swelling. Spine: Inspect following movement by viewing the affected person from following positions: From behind From facet Ask the affected person to bend forward Ask the patient to touch chin on the chest Ask the patient to the touch his chin to the shoulder. Ask Recording of findings: If gait is normal, information of bodily finding obtained from above examinations are normally regular. Muscles Examination Wasting: Measure the circumference of limb and compare with the other limb. Washing could also be: Associated with joint disease: Washing of small muscles of the hand in rheumatoid arthritis Washing of quadriceps in arthropathy of the knee Without joint illness: Primary muscle disease Myasthenia gravis Normally in elderly folks however not accompanied by weakness. Increased muscle bulk: the muscle tissue of the physique could additionally be actually hypertrophied as a end result of increase in muscle bulk: It could be seen in a body builder. Spontaneous muscular contraction: Spontaneous actions of the muscle tissue can occur in: Upper motor neuron disease-flexor or extensor spasms of legs muscles at hip or at knee. Fasciculation occurs in single muscle could also be due to: Physiologically primarily confined to calves. If the muscle is tender: Alcoholic myopathy Myositis Peripheral neuropathy produced by thiamine deficiency. Testing of muscle power: Regarding testing of muscle power following questions should be necessary: Whether weakness in focal or global Spine examination: Cervical backbone: � Seven cervical vertebrae � Five intervertebral disc (C 2/3�C 6/7) � C7/T1 disc is related to radicular symptoms � Degenerative disease frequent between C5 and T1 disc � C2 and C3 nerve root covers sensation again of the top, decrease jaw line � C4 to T1 nerve roots produces bacterial plexus. Lumbar vertebrae: � fifth lumbar vertebrae � Transition between cell lumbar spine and stuck sacrum along with excessive weight loading mix to make the region highly prone to break. Nerves then run individually in the spinal canal-they together are termed as caudal equine. There are secondary curvatures rely upon anterior and posterior aspect of intervertebral disc. These are primary curvature-determined by anterior and posterior facet of intervertebral disc at these ranges. Maximal on the junction of atlas and occipital bone lumbar vertebral In Cervical vertebrae. Lateral flexion: Greatest at atlantoaxial area some extent in lumbar and cervical area To Least movement in thoracic region. Examination of backbone at total: Ask the affected person to face erect-watch the posture of the affected person: Increased flexion-Kyphosis. As the spinous course of rotates in the direction of midline, scoliosis is accentuated when the affected person bends forwards. Examination of cervical spine: this ought to be examined when the patient is in sitting positions. Examine passive actions of cervical spine: � Ask the patient to the touch his chin to chest-flexion. Remember the motion of neck-the vary movements relying on age, intercourse and ethnicity. Normal vary of lateral flexion is 45� and rotatory movement is 70� in normal middle aged particular person. Neurological examination of upper and decrease limb for any paresthesia, washing, weakness, exaggeration of reflexes, clonus, plantar response. Examination of thoracic backbone Inspection: Patient ought to be inspected from back and front: Scoliosis-it could also be: Note Musculoskeletal System 1329 Nonstructural because of back ache or stomach pain, leg length discrepancy Psychogenic or Structural-due to bony lesions. Marked kyphosis may be due to: Osteoporotic vertebral fracture Degenerative disease. Loss of regular kyphosis-flat spine could also be as a outcome of: Spondylotic changes Severe muscle spasm. Costochondral swelling-may be because of: Costochondritis Synovits of costosternal joint and sternoclavicular joint. Range of thoracic motion is: 30� extension 20��40� lateral flexion 25��45� flexion 30��45� rotation. Chest expansion-from forced expiration to compelled inspiration could be measured by tape-which is in regular individual no much less than 5 cm. Other examinations Neurological examination of lower limbs to see any signal of spinal twine compression. Note: Any hyperlordosis (L5�S1 damage) Prominent thoraco lumbar kyphosis (multiple disc degeneration, vertebral fracture). Lateral flexion: Legs and again straight, strikes sideways along with his hands down the side of the thigh. Flexion could be mediated by hip joint and extension could be affected by slight pelvic tilt. Disease Interpretation Pain on extension: Retrospondylolisthesis Facet joint arthritis. Failure of spinous process to separate throughout flexion- Parmanent spinal stiffness-ankylosing spondylosis. Ask the patient to face on one foot then to their toes in few occasions-weakness could also be because of L5 nerve root entrapment. Gait pattern the next are the abnormalities of the gait: Antalgic gait Wise base gait: Muscular weakness Cerebellar deficit Short shuffling gait-Fastinant gait-Parkinsonism Gait of old age-lean ahead and small steps Flat ft Feet valgus Genu recurvatum. Flex the leg at hip and then prolong the legs at knee in order that higher leg is vertical. Lift one leg, flex and abduct on the hip barely, whereas different limb kept in extended position. Deviation from regular Normally, there could additionally be tightening because of posterior thigh or calf muscles. Fallacy this take a look at will not be positive even the affected person may be suffering from sciatica. When central constructive dire prolapse occurs-may be unfavorable: Testing muscular tissues of decrease limb: Hamstrings (L5 S1 S2)-Knee flexion: Ask the patient to flex the legs on the knee to 45�, and also you give resistance from reverse facet to flex the knee. Iliopsoas (Hip flexor and internal rotator)-L1, L2, L3: Ask the patient to flex the limb at the hip and rotate internally. Now ask the affected person to straighten the lower legs against resistance given by your palms.
These issues can be broadly categorised into benign or invasive/malignant (see Box eight erectile dysfunction doctors in nj buy generic top avana line. Research has shown related charges of future intrauterine being pregnant and recurrent ectopic rates compared with medical management erectile dysfunction 43 discount top avana. Salpingostomy (incision of the affected tube with elimination of the merchandise of conception) is occasionally performed with a view to growing future intrauterine pregnancy rates erectile dysfunction and coronary artery disease in patients with diabetes purchase 80 mg top avana visa. Invasive moles follow roughly 15% of complete moles and 3% of partial moles impotence used in a sentence purchase top avana pills in toronto. Choriocarcinoma is a malignant disease characterised by abnormal trophoblastic hyperplasia and anaplasia erectile dysfunction treatment medicine cheap top avana 80 mg on line, absence of chorionic villi iief questionnaire erectile function order 80mg top avana amex, haemorrhage and necrosis. There had been multiple pulmonary metastases however restoration was full after hysterectomy. The condition is more common in Australasia (1 in 750 pregnancies) than within the United States, the United Kingdom and Europe (1 in 1500), but is most frequent in South-East Asia and Mexico (1 in 500). Typically, a mole is initially identified following an ultrasound performed because of vaginal bleeding (95%) in early being pregnant. Complete molar pregnancy occurs on account of fertilisation of an empty ovum with either two sperm or one which divides. Choriocarcinoma the clinical presentation of choriocarcinoma is diversified relying on the antecedent being pregnant. Following a traditional being pregnant, persistent vaginal bleeding is the most frequent symptom. There may be evidence of metastatic tumour-vaginal metastases are present in 30% circumstances. Patients may exhibit respiratory, gastrointestinal or neurological symptoms reflecting sites of distant metastases. Occasionally, the prognosis of a partial mole may solely be made on histology of curettings from a suspected incomplete abortion. Heavy bleeding may complicate this course of, so adequate blood must be crossmatched. Suction curette is first-line management for full and partial molar being pregnant. The fetus and attached placenta had a traditional male karyotype however the separate molar tissue had a female karyotype and was thus a dizygotic twin. The theca lutein cysts are managed conservatively though they might take months to resolve. The single placenta was diffusely molar and the triploidy fetus had multiple abnormalities. Tissue is sent in regular saline (not formalin) for histological analysis and karyotyping if essential. Repeat curette is contraindicated because of the significant threat of maternal haemorrhage and uterine perforation. For high-risk disease necessitating a multi-drug routine ± adjuvant radiotherapy or surgical procedure, treatment charges are roughly 90%. Outcome of expectant management of spontaneous first trimester miscarriage: observational research. Gestational trophoblastic illness I: epidemiology, pathology, clinical presentation and analysis of gestational trophoblastic illness, and administration of hydatidiform mole. A comparability of medical management with misoprostol and surgical administration for early pregnancy failure. Congenital defects may be because of genetic, infective or teratogenic influences, but the aetiology in plenty of stays unknown. Screening for delivery defects contains screening for Down syndrome and related aneuploidies, and a fetal anatomical survey with ultrasound. Other genetic circumstances in high-risk families could also be amenable to prenatal screening and analysis. Diagnostic tests for genetic abnormalities embrace amniocentesis and chorionic villus sampling, which have a miscarriage rate of zero. Cardiovascular and central nervous system abnormalities are the most typical major structural abnormalities; nonetheless, renal, gastrointestinal, face and skeletal abnormalities may be detected with ultrasound, as might fetal tumours or hydrops. Management of families where a significant structural abnormality has been identified is finest undertaken by a multidisciplinary team addressing: the underlying trigger; implications for the pregnancy, labour and supply; newborn care and long-term prognosis; danger of recurrence; and options for the pregnancy, including continuation versus termination of the being pregnant. Many congenital defects have a genetic origin, whether from chromosomal defects (approximately 10%), single gene issues (approximately 5%) or where inheritance is multifactorial (approximately 25%). Other defects could also be a result of fetal infection, corresponding to toxoplasmosis, rubella, cytomegalovirus and herpes simplex virus (see Ch 19) or publicity to recognized teratogens. Screening for other genetic disorders with essential well being implications however with no recognisable phenotype on ultrasound may be performed for disorders such as thalassaemia, cystic fibrosis and fragile X syndrome. Management of pregnancies where the fetus is understood to have a fetal abnormality or severe medical condition requires the involvement of a multidisciplinary group. Counselling should address the implications of the prognosis for the remainder of the being pregnant, labour and delivery, Chapter 9 Screening, Diagnosis and Management of Genetic and Structural Abnormalities within the Fetus for postnatal care and the long-term implications. Some situations could also be amenable to in utero treatment, while most will contain postnatal surgery, medical therapy or ongoing surveillance. In some situations, the place the outlook is lethal, palliative care may be offered to the new child. In situations the place a fetus is recognized with a severe or life-threatening condition, some families could contemplate adoption, while many will face the tough determination of pregnancy termination. It is the commonest chromosomal abnormality related to reside birth, and the main explanation for mental incapacity related to a recognisable chromosomal abnormality. Up to 50% of newborns may have congenital heart disease and different structural abnormalities which might be identified prenatally, together with duodenal or oesophageal atresia. Medical issues embrace hypothyroidism, listening to and eye abnormalities, and an elevated danger of some malignancies. Behavioural and psychiatric problems are more widespread, in addition to autism and early-onset dementia. Down syndrome affects approximately 1:600 to seven-hundred pregnancies, although this is decided by the maternal age of the inhabitants being studied, because the majority of pregnancies affected by trisomy 21 occur as a result of nondisjunction. Trisomy 21 from nondisjunction happens when one gamete contributes 24 chromosomes (including two copies of chromosome 21) to the conceptus as a substitute of the usual 23, leading to 47 chromosomes. The majority of nondisjunction events are maternal in origin, and are more frequent with rising maternal age. This explains the elevated risk of miscarriage as a end result of aneuploidy, and of stay birth with Down syndrome, noticed in older ladies. Less than 5% of instances of Down syndrome occur on account of translocation, where the lengthy arm of chromosome 21 is connected to another chromosome, normally chromosome 14. While the translocation is balanced (with a traditional and complete complement of genetic material within the carrier parent), this has the potential to become unbalanced on the time of conception. Historically, maternal age was the only screening take a look at supplied for Down syndrome, with all women aged 37 and over on the time of supply provided invasive testing. However, this leads to a screen positive fee of roughly 10% for a Down syndrome detection rate of solely 30%. Population-based screening packages using serum screening, ultrasoundbased screening or a mix of both have vastly improved detection charges of Down syndrome, and it is strongly recommended that every one ladies be provided a screening take a look at, regardless of maternal age. After Down syndrome, the chromosomal abnormalities more than likely to end in reside delivery are trisomy thirteen and trisomy 18, although both are nearly inevitably deadly. Gestation-specific reference ranges have been established and so maternal serum screening outcomes are expressed as multiples of the median (MoM). The likelihood ratio comparable to the maternal serum MoM is utilized to the maternal a priori threat (the danger associated with her age alone) and a model new threat is generated. The more maternal serum analytes that are examined, the upper the Down syndrome detection rate. When screening incorporates all 4 analytes, the detection rate in well-dated pregnancies is roughly 75% utilizing a cut-off of 1:250 or larger and a false-positive price of 5%. This signifies that 5% of ladies will display optimistic, having an adjusted individual risk result between 1:2 (highest possible screen-positive risk) and 1:250 (lowest possible screen-positive risk), but nearly all of these will turn out to be false-positives. The drawback of this check is the later gestation on the time of testing, and that the pregnancy needs to be precisely dated. While this take a look at has comparable accuracy to second-trimester maternal serum screening, the advantage is the elevated privacy supplied by earlier screening; most families and clinicians would favour first-trimester screening and prognosis. For this cause, the Fetal Medicine Foundation provides solely accredited sonographers with entry to the software program bundle that generates the personalised risk. With first-trimester mixed screening, patients have a blood check carried out at 9 to 12 weeks followed by an ultrasound at eleven to 13 weeks (see earlier section). The adjusted danger displays the likelihood ratio generated by each the maternal serum screening and nuchal translucency results utilized to the background maternal age risk. Not surprisingly, utilizing the modalities of both ultrasound and maternal serum screening leads to an improved sensitivity; the detection fee utilizing first-trimester mixed screening is roughly 90% at a cutoff of 1:300 and a false-positive rate of 5%. This ultrasound is carried out when the crownrump size measures forty eight to eighty four mm, comparable to a gestational age of 11 to thirteen weeks. A Normal nuchal translucency, measured with a well-magnified image, separate to the amnion and the neck in a impartial position. This minimises the risk of requiring a diagnostic test, with the attendant procedural loss, while retaining maximal sensitivity. In the previous strategy, high-risk ladies on the idea of the firsttrimester results. In the latter approach, three ranges of risk are recognized at the finish of first-trimester testing: high-risk ladies. Nevertheless, such soft markers are present in roughly 15% of normal pregnancies, and so use of ultrasound alone as a screening test is insufficient. Ultrasound analysis for structural abnormalities and delicate markers may be utilized in mixture with maternal serum screening with detection charges for Down syndrome rising from approximately 80% to 90% on this setting. A regular second trimester ultrasound is related to roughly halving the risk generated by maternal serum screening alone. Abnormal maternal serum screening results: different implications Very irregular maternal serum results could also be seen in a variety of different pregnancy problems, even when the adjusted aneuploidy threat is low or chromosomal abnormalities have been excluded with diagnostic testing. Second trimester An elevated maternal serum alpha-fetoprotein in the second trimester (> 2. The finding of a maternal serum alpha-fetoprotein in this range should immediate a tertiary-level morphology ultrasound to exclude these and other structural defects. If no abnormality is confirmed, progress surveillance is really helpful in late pregnancy. While initially only really helpful for high-risk women, this technology has quickly transitioned into medical apply, and huge datasets are confirming wonderful take a look at performance characteristics in low-risk women. Confirmation with invasive testing continues to be necessary for sufferers with a display positive end result. Given the comparatively high cost of this check, applicable counselling is important for sufferers wishing to consider non-invasive prenatal prognosis to ensure the constraints of this take a look at, together with failed fetal fraction, and the potential for atypical findings are understood. A gentle marker is a bodily 74 Diagnostic tests Among ladies who screen as high threat for aneuploidy, the available diagnostic exams are chorionic villus sampling and amniocentesis. The process is mostly performed between 12 to 14 weeks and is commonly the diagnostic test chosen after abnormal firsttrimester screening. Information that could be obtained from the genetic materials taken at diagnostic testing contains fluorescent in-situ hybridisation, banded karyotype, microarray and single gene testing. This is a take a look at the place fluorescent-labelled probes attach to critical areas on individual chromosomes. Standard karyotyping includes examination of all chromosomes and can diagnose · · · issues of chromosome quantity (aneuploidy) or structure, corresponding to deletions, duplications and translocations. Microarray evaluation allows detection of chromosomal deletions or duplications which are one hundred instances smaller than those recognized on standard karyotype. Nevertheless, microarray analysis carries the potential for findings of uncertain significance, and consultation with a genetic counsellor with consideration to pre- and posttest counselling is beneficial. This may be carried out on any prenatal sample for autosomal-dominant, recessive or X-linked circumstances the place the genetic defect is thought. This means the delivery prevalence for cystic fibrosis is 1:2500 (1:25 Ч 1:25 Ч 1:4). Cystic fibrosis is a dysfunction of exocrine gland secretions inflicting an accumulation of thickened secretions that result in recurrent lung infections, malabsorption, infertility in males and shortened life expectancy. Antenatal screening includes performing a cheek swab or blood check to check for the most common genes liable for cystic fibrosis. Diagnostic testing may be performed where both parents are confirmed to be carriers, the place the danger to the fetus is 1:four. Alpha-thalassaemia major (where all 4 genes coding alpha globin synthesis are missing) is incompatible with life since alpha chain synthesis is important for all haemoglobin varieties. Beta-thalassaemia main is associated with lifelong transfusion-dependent anaemia, a need for chelation therapy and shortened life expectancy. Families must fastidiously weigh up the additional data obtained regarding their pregnancy towards the financial value and anxiousness generated by sudden findings. Genetic counsellors are invaluable in assisting with pre- and post-test counselling. Other genetic conditions Advice should be sought from a prenatal genetic counsellor relating to the place for prepregnancy or antenatal screening of other high-risk teams. Examples embody screening of Ashkenazi Jews for Tay Sachs disease, and screening for Fragile X among households with a historical past of male autism or mental incapacity or those with a identified household historical past of genetic circumstances. Prepregnancy identification of high-risk couples permits them to think about assisted reproductive choices corresponding to preimplantation genetic analysis or use of donor gametes to minimise their risk of an affected child. Women with diabetes have an increased risk of malformations, with the risk immediately correlated with Hb A1C on the time of conception. Obesity is associated with a Chapter 9 Screening, Diagnosis and Management of Genetic and Structural Abnormalities in the Fetus small but considerably elevated risk of some structural abnormalities. Prevention of structural abnormalities thus consists of advice on optimising drugs, diabetic management and weight prior to being pregnant. Folic acid should be prescribed to all girls considering being pregnant, and high-dose folate (5 mg daily) for ladies at elevated danger of neural tube defects.
Supraoptic portion: � Supraoptic nuclei � Suprachiasmatic nuclei � Paraventricular nuclei xyzal impotence buy top avana 80mg on line. Tuberal portion: � Ventromedial nuclei � Dorsomedial nuclei � Arcuate nuclei � Medial eminence stress and erectile dysfunction causes buy cheap top avana 80 mg line. Mammillary portion: � Premammillary nuclei � Medial mammillary nucleus � Lateral mammillary nucleus � Posterior hypothalamic nucleus erectile dysfunction causes heart disease order discount top avana online. Curling up Decreased Cutaneous vasoconstriction Heat Horripilation Loss Mechanisms activated by heat Cutaneous vasodilatation Increased Increased sweating Heat Increased respiration Loss Anorexia Decreased Apathy Heat Production Subthalamus Subthalamic nucleus or physique of Luys medial to inside capsule erectile dysfunction ugly wife buy top avana now. Ventrolateral portion-Field H2 Epithalamus It consist of: Habenular trigone: It incorporates: Habenular nuclei: It receives fibers from stria medullaris thalami Habenulopeduncular tract: It extends from habenular nuclei to interpeduncular nucleus in midbrain erectile dysfunction in diabetes medscape buy 80 mg top avana amex. Pineal physique Tumor of pineal body-obstructs cerebral aqueduct erectile dysfunction natural shake buy top avana cheap online, or incapability to maneuver eyes in vertical plane-Parinaud syndrome Other tumor-Germinoma: It produces precocious sexual development. Posterior commissure: this band lies on the boundaries between diencephalon and midbrain. Temperature regulation Afferent from Cutaneous chilly receptors, temperature delicate cells in hypothalamus 865 Integrating areas Ant hyp: Response to warmth Post hyp: Response to cold 2. Hunger Emotional stimuli through limbic system Osmoreceptors � volume receptors Touch receptors in breast, uterus, genitalia Temperature receptors i. Suprachiasmatic nuclei (diurnal rhythm) Hypothalamic cells delicate to estrogen Touch receptors in breast, different unknown receptors Unknown receptors Dorsomedial and posterior hypothalamus Supraoptic and paraventricular nuclei Supraoptic and paraventricular nuclei Dorsomedial nuclei Paraventricular nuclei Preoptic areas Arcuate nucleus, other areas (hypothalamus inhibits secretion) Arcuate nucleus, periventricular nucleus Ventromedial satiety center, lateral starvation heart Anterior and ventral hypothalamus in male, piriform cortex Supraoptic hypothalamic nuclei j. Parieto-occipital fissure: It passes alongside the medial floor of the posterior portion of cerebral hemisphere, separates parietal lobe from occipital lobe. Calcarine fissure: It presents on the medial floor of the hemisphere close to occipital pole. Circuminsular fissure: It surrounds insula and separates it from frontal, parietal and temporal lobes. Carpus Callosum Large myelinated bundle of fibers: It crosses longitudinal cerebral fissures and interconnects giant parts of cerebral hemispheres. Neurology 867 Frontal Lobe Gyri Superior frontal gyrus Middle frontal gyrus Interior frontal gyrus: It is divided into three parts from anterior: 1. Opercular portion Precentral gyrus parallel to central sulcus Orbital gyrus Straight gyrus Cingulate gyrus Paracentral lobule-quadrilateral gyrus-around the tip of central sulcus on medial surface of cerebral hemisphere. Parietal Lobe Gyri Postcentral gyrus Superior parietal lobule Inferior parietal lobule Supramarginal gyrus: It arches above the ascending end of the posterior ramus of lateral fissure Angular gyrus: It arches above the tip of superior temporal sulcus Precuneus: It is present on the posterior portion of medial floor. Sulcus Postcentral sulcus Interparietal sulcus dividing superior and inferior parietal lobule. Occipital Lobe Lateral occipital sulcus extends transversely and divides occipital lobe into: Superior gyrus Inferior gyrus. Calcarine fissure divides medial surface of occipital lobe into: Wedge-shaped cuneus Lingual gyrus. It lies deep in cerebral fissure Short gyri: It lies on anterior portion of insula Long gyri: It lies on posterior portion of insula. White Matter in Cerebrum White matter accommodates myelinated nerve fibers of many sizes. Anterior commissure: It connects two olfactory bulbs and temporal lobe constructions. Projection fibers: these fibers join cerebral cortex with lower portions of mind and spinal wire. Two primary forms of association fibers: Short affiliation fibers (U fibers): these connects adjoining gyri: � Intracortical fibers: It is situated in deeper portion of cerebral cortex � Subcortical fibers: It is positioned just beneath the cortex. Long association fibers: It connects extensively separated areas � Uncinate fasciculus: It connects the interior frontal lobe gyri with anterior temporal lobe � Cingulum: White band mendacity within cingulate gyrus, connects anterior perforated substance with parahippocampal gyrus � Arcuate fasciculus: It connects superior and center frontal gyri to temporal lobe and frontal pole � Superior longitudinal fasciculus: It connects parts of frontal lobe with occipital and temporal areas � Inferior longitudinal fasciculus: It connects temporal and occipital poles � Occipitofrontal fasciculus: It connects frontal lobe with temporal and occipital lobes. Parietal lobe: Area three, 1, 2-Primary sensory areas Area 5, 7-Sensory affiliation areas Area 39, 40-Association areas. Temporal lobe: Area 41-Primary auditory areas Area 42-Auditory affiliation areas Remaining areas-Association areas. Occipital lobe: Area 17-Primary visible cortex Area 18 and 19-Visual association areas. Afferent tract Putamen and globus pallidus receives some fibers from substantia nigra Thalamus sends fibers to caudate nucleus. Anterior limb: It accommodates: � Thalamocortical and corticothalamic fibers be a part of lateral thalamic nucleus and frontal lobe cortex � Frontopontine tract connecting frontal lobe to pontine nuclei � Fibers from caudate nucleus to putamen. Central part: � Corticobulbar tract � Corticospinal tract � Corticorubral tract from frontal lobe cortex to purple nucleus. Retrolenticular part: Thalamocortical tract-from posterolateral nucleus of thalamus to postcentral gyrus. Sublenticular half: � Parietotemporopontine tract: It is connecting parietal lobe, temporal lobe cortex to pontine nuclei � Auditory radiations: Fibers from medial geniculate physique to transverse temporal gyrus � Optic radiations: Fibers from lateral geniculate physique to visible cortex. Vertebral Arterial System Supplies Cerebellum Brainstem Occipital lobe Part of thalamus. Two vertebral arteries are joined to type a basilar artery-it ends by forming two posterior cerebral arteries. Anterior cerebral artery of one hemisphere is joined with the same of opposite aspect by anterior communicating arteries. Vertebral arteries and basilar arteries give a number of branches: Anterior-inferior cerebellar arteries Posterior-inferior cerebellar arteries Superior-cerebellar arteries Pontine arteries Internal auditory arteries Perforating arteries. Anterior Cerebral Artery and Its Branches Supplies Anterior frontal lobe Medial aspect of hemisphere A strip of cortex spanning its superior margin. Right auditory cortex is specialized for spectral processing (responsible for analyzing musical sounds) and gradual processing mode Right frontal lobe is bigger than the left frontal lobe. Left occipital lobe is larger than the proper occipital lobe Neurology 875 Right hemisphere is dominant for: Skillful task Constructional abilities Nonvisuospatial perception � Somesthetic � Auditory (Melody and tone discrimination) � Emotional functions-comprehension of emotional tone, voice and physique gestures. Retrorolandic potion of cerebral hemisphere (postcentral gyrus) is involved in processing sensory information of outdoor world and concerning the motor act carried out by particular person. The latter motion requires integration of different modalities of sensations (visual, somatosensory, auditory). Cortex-adjacent to main sensory area is called secondary sensory cortex-process unimodal sensory info Cortex-lying between completely different secondary sensory areas are referred to as tertiary sensory cortex-responsible for processing multimodal sensory info. Example: Somatosensory data reaches somatotopically to postcentral gyrus, which projects somatotopically upwards to superior parietal lobule (arm and leg) and downwards to inside parietal lobule (head). Somatosensory information is built-in with auditory and visible information in angular gyrus. With visual in vegetative information in precuneus (posteromedial portion of parietal lobe). For example, bilateral lesions in posterior portion of superior parietal lobule result in impairment of hand movement beneath visible steerage. Activation of major, secondary and multimodal sensory areas are stimulus particular and contact specific. For instance, Activation of left posterosuperior temporal gyrus is activated by acoustic adjustments in speech and nonspeech sounds Activation of left supramarginal gyrus is engaged in detection of modifications in phonological models. Activation of sensory areas are modulated by prefrontal cortex, cingulate cortex, insular cortex Prerolandic portion of cortex is liable for planning, initiation and execution of actions in a meaningful means, 876 Clinical Methods and Interpretation in Medicine getting data from the realm of mesial frontal cortex (cingulate gyrus and supplementary motor areas) linked with reticular activating system and limbic lobe. Precentral gyrus is responsible for nice distal actions whereas subcortical structures are responsible for axial actions. Cerebellum, brainstem and vestibular complexes are liable for important feedback info. Regarding Lesions in Cerebral Hemisphere Lesions involving cerebral hemisphere is much less pronounced than comparable volumes of lesion involving brainstem because of: Redundancy of pathways Plasticity of hemisphere Large variety of cortical neurons. Neurological deficit brought on by cerebral hemisphere lesions is inconsistent than deficit involving lower brainstem Patient could also be unaware of extent and high quality of deficit especially when it includes multimodal behavior (apraxias, aphasia). Same operate is represented in numerous areas of cortex and contralateral hemisphere in numerous sufferers Hemispheric features are subserved by: Extensive networks Hence, single lesion could also be silent and turns into symptomatic when extra areas will be concerned impairing network functions. Neurology 877 A related quantity of tissue may be responsible for global aphasia in acute state, however, becomes answerable for motor aphasia few weeks later-it could also be because of: Perilesional edema Metabolic abnormalities Dysfunctions of the areas of mind away from the broken space of mind. Lesions affecting same parts of cerebral hemisphere current with variable medical pictures depending upon nature and tempo of lesion. For instance, Infarcts-small infarct in brain produces aphasia in acute presentation. Cortical plasticity results is extra or less complete recovery from elemental motor and sensory deficit, though extra complicated motor or sensory deficits remain-this happens as a result of useful reorganization of cortex-so that sound cortical area take over the capabilities of lesioned cortical area. In case of subcortical lesions, the newly organized space, when firstly developed, turn out to be larger than the lesioned space. Cortical plasticity is mediated by multicentric arrays which are vulnerable to metabolic insult-as a outcome, processing and elaboration of neurotransmitters might be hampered. Lesions involving cortex (hypoxic laminar necrosis)-giving rise to clinical picture-that differs from medical image produced on account of lesions involving white issues (multiple sclerosis). Characteristics of cortical lesions Seizures Multimodal motor and sensory deficits. Characteristics of white matter lesion Weakness Spasticity Pure motor syndromes Urinary incontinence Visual area deficit. This motor efficiency is determined by: Level of alertness, mediated by ascending reticular activating system Cortical consideration Perception of sensory stimuli and their relation with past experiences the flexibility to carry out sequence of events-those make up motor act itself. The following clinical features are helpful in neurological diagnosis: Distribution of weak point Unilateral or bilateral Symmetrical or asymmetrical Primary proximal or major distal. Presence or absence of sensory symptom Type of distribution Unilateral or bilateral. Presence or absence of pain Presence or absence of cranial nerve abnormalities Presence or absence or exaggeration of reflexes Presence or absence of pathological reflexes Involvement of bladder and bowel disturbances Presence or absence of signs relating to cortical involvement. The stage of lesion could also be in: Muscle Neuromuscular junction Peripheral nervous system Nerve roots Spinal cord Brainstem Hemisphere. Cerebellar Disease Signs of cerebellar disease-Tremor, in co-ordination, ataxia, vertigo, dysarthria, difficulty in walking and nystagmus No muscle weak spot No sensory loss 880 Clinical Methods and Interpretation in Medicine Normal reflexes No pathological reflexes No sphincter dysfunction No cortical dysfunction. Cortical and Subcortical Involvement Unilateral cortical involvement often produces hemideficit within the form of: hemiparesis hemisensory deficit hemianopsia hemiseizures. Hyper-reflexia Pathological reflexes-Babinski response No bladder-bowel involvement-till bilateral cortical involvement will happen If thalamus is involved-pain might be a function If dominant hemisphere is involved: Language disturbances like-agraphia, alexia, and aphasia will occur If nondominant hemisphere is involved-agraphia If any cortical hemisphere is concerned: Astereognosis, impaired two factors discrimination, memory defect, cognitive defect If subcortical buildings are involved: Hemidistribution of dysfunction apart from agraphia, language disturbance, cognitive defect, seizures. Common causes of muscle disease Muscular dystrophies Inflammatory Toxic Metabolic Congenital. Common causes of neuromuscular junction disorders Myasthenia gravis Eaton-Lambert syndrome Neurology 881 Botulism Hypermagnesemia. Common causes of peripheral neuropathy Guillain-Barr� syndrome Alcoholism Diabetes mellitus. Common causes of plexus illnesses Trauma Neuralgic amyotrophy: Parsonage-Turner syndrome Plexitis. Common causes of spinal twine illness Transverse myelitis Trauma Infective-tuberculosis. Some problems could contain more than one locations Devic illness Involvement of optic nerve Involvement of spinal twine. Amyotrophic lateral sclerosis: Involve spinal wire to cerebral cortex-spares sensory operate and cortical perform. During above type of questioning-you may need to do few main questions-like: Pricking type ache or knife like pain Throbbing or bursting sort of headache Associated blurring of vision, nasal congestion, and so forth. Exaggeration and remission of symptoms with progressive improve in severity of symptoms in each exacerbation- Multiple sclerosis. Comparatively sudden with or with out fever, gradual deterioration followed by progressive recovery if affected person will get proper remedy. But if time of commencement of remedy is delayed, complete restoration might not occur. Recent earlier historical past could also be necessary in some instances to get mild in the present illness. Trauma Hypertension Neurology 883 Vascular occasions Demyelinating diseases-like episodes of visual loss-within 3�5 years-may strengthen the recent symptoms. Past Medical Relevant History Following history could additionally be related: History of trauma Operation Chronic illness Hospitalization Accidents Infectious illnesses Venereal illnesses Over the counter drugs. Muscle disease Symmetrical proximal Absent Intact but in severe circumstances absent Bladder or bowel disturbances Normal 2. Neuromuscular junction Absent Normal in Myasthenia gravis Depressed in Eaton-Lambert syndrome Nil Normal Normal three. Peripheral neuropathy Symmetric and proximal may be bulbar involvement (1) Eye movement weakness- producing double vision or ptosis, (2) Dysphagia, (3) Nasal regurgitation of fluid Symmetric and predominantly distal sort may be proximal Nil Normal Normal Present Depressed or absent Pain may be present Clinical Methods and Interpretation in Medicine Contd. Level Weakness of muscle Sensory loss Deep tendon reflexes Nil Normal Normal Pathological reflexes Bladder or bowel disturbances Cortical perform Other symptoms four. Nerve root disease Motor weak point Sensory loss Depressed in the Nil distribution of root Pain along the distribution of root- aggravated by movement of neck or low again ii. Brainstem illness Hyperactive Crossed cranial nerve May or may on the aspect of lesion not be present and weakness of limb on opposite side If posterior fossa structure is concerned � vertigo, ataxia, dysphagia, nausea, vomiting, abnormal eye actions Neurology Alcoholism 887 Abuse of medicine. In few instances, pes cavus, stork-leg deformities could have a family relation but in this case, the historical past taking is being neglected since these illnesses are quite common amongst folks. Relevant Social History Social history contains: Marital standing Number of marriages Duration of present marriage Any disturbance in marital adjustment Health of the wife and youngsters. Occupational standing Present occupation Working environment Any private protection throughout working time Level of exertion the affected person is no longer working-when and why he stopped. If Hobbies: Enquiry concerning hobbies or avocations Personal habits Use of alcohol, tobacco, road drugs, espresso, tea or delicate drinks Any abstinence Cause of abstinence. Have you ever had a morning eye-opener to regular your nerves or get rid of a hangover Abuse of inhaling much less refined substances-spray paints, paint thinner, gasoline, airplane glue. Enquiring about following Symptoms in a Suspected Neurologic Patient Headache Loss of consciousness: It may be mainly due to: a. Neurology 889 Ataxia Any affected person having dizziness-must be evaluated for abnormal functions of vestibular, ocular, cerebellar and proprioceptive systems-equilibrium requires the combination of sensory input and motor output to maintain up balance.
Syndromes
Stopping smoking
An abnormal finding on an x-ray or bone scan
Difficulty breathing
The most common type of contrast given into a vein contains iodine. A person with an iodine allergy may have nausea or vomiting, sneezing, itching, or hives from this type of contrast.
Whether a previous vaccine helped your immune system protect you against the specific disease
Axillary nerve dysfunction
Twitching in face
Nausea and vomiting
Tricyclic antidepressants
Anterior cruciate ligament: It attaches above to the femoral lateral condyle and is inserted into the tibial backbone through a slip hooked up to the anterior horn or lateral meniscus best erectile dysfunction doctors nyc safe top avana 80 mg. Posterior cruciate ligament actions: It stabilizes the joint by preventing ahead displacement of femur relative to tibia erectile dysfunction doctor philippines discount top avana 80 mg otc. Medial collateral ligament: It stabilizes the knee from valgus stresses, during flexion erectile dysfunction bangalore doctor top avana 80mg low price. Patella: It is a sesamoid bone-it is present and articulates with femoral condylar groove, it makes quadriceps action more efficiently erectile dysfunction at age 23 purchase top avana 80mg free shipping. Examination of Knee Joints Inspection and Palpation In affected person with standing position Deformity: Knock knee-genu valgum where each the knees are available in contact with each other erectile dysfunction nclex discount top avana 80mg on-line. Ask the affected person to increase the knee actively-the motion should be smooth, ache free erectile dysfunction drugs stendra order generic top avana from india. If rotation is abnormally excessive, then medial collateral ligament is both poor or form. Tenderness to tibiofemoral joint delicate for: Meniscus tear Appearance of osteophytes Patellofemoral joint tenderness can be elicited by giving gentle stress down the patella. Causer of patella femoral joint tenderness: High patella Excessive pronation Weak vastus medialis Reduced movement on the ankle Wide Q-angle. Then gently press the patella into the femur down ward by 2nd and third finger of proper hand. Then with index and center finger of proper hand, give mild stroke in between patella and femoral condyle. Thickened synovium could be palpated by wrapping the finger around beneath the knee in semiflexed position to the knee. Ask the patient to lie flat with hip flexed and knee flexed at 90�, and foot ought to be flat on the bed. Now sit on the foot of the affected person and check out to attract the upper end of tibia forwards within the line of thigh. Ask the patient to lie flat with hip flexed and knee flexed at 90� with foot lie flat on the mattress. Now sit on the foot of the affected person and try to push the higher tibia backwards along the line of thigh. In osteoarthritis: Tenderness at the insertion of capsules and collateral ligament is essential. Examination of muscular tissues involving the knee joint movement: Both quadriceps weakness and wasting-accompanying joint illness. Causes of femoral neuropathy Trauma Hemorrhage within the psoas sheath Diabetes mellitus. In femoral neuropathy: Weakness and losing of femoral quadriceps Loss of knee jerk Sensory changes over anterior thigh and medial side of decrease leg. In case of obturator nerve palsy: Weakness of thigh adductors Altered sensation on the internal side of the thigh. Meralgia paresthetica: the most common entrapment neuropathy Causes: Compression of the lateral cutaneous nerve of thigh on the degree of groin. Signs and signs: Pain, tingling numbness over anterolateral side of the thigh. Strong ligaments-secure: Tibiofibular joint at decrease end Talocalcaneal joint Bones of midfoot. Movement and vary of motion in numerous joints Ankle joint: 50� plantar flexion 20� dorsiflexion eversion 5� inversion. Evertors of foot Peroneus longus-inserts into medial cuneiform-acts as everters of foot Peroneus brevis-inserts into fifth metatarsal bone-acts as everter of foot. Deeper layers-include: Interossei of forefeet Tibialis posterior Peroneus longus Adductor hallucis Flexor hallucis brevis-it has two insertions into proximal nice toe phalanx. Superficial layers: Flexor digitorum longus Lumbricals Flexor digitorum brevis Abductor hallucis. Arches: Longitudinal arch-apex on the talus Transverse arch-apex at medial cuneiform-It keep, stabilize the foots. Skin over dorsum of foot Supplies: Tibialis anterior Extensor hallucis longus Extensor digitorum longus It runs within the posterior lower leg-supplying a. Skin: the following pores and skin lesions could be demonstrable: Purpura Panniculitis Erythema Pyoderma gangrenosum (mainly seen over shins). Swelling around the fibular head in patient with foot drop- widespread peroneal nerve palsy. Examination of Ankle and Hindfoot Thickened tissue around ankle joint and round mutely-ankle joint arthritis. If posterior tibial or perineal tendon are inflamed-there is soft tissue swelling of medial and lateral hindfoot, there could also be related involvement of talocalcaneal joint. Twisting of midfoot: Rheumatoid arthritis Spondyloarthropathy, gout Nonspecific Tenderness on bone without gentle tissue involvement-does not exclude synovitis Midfoot arthropathy-typical of neuroarthropathy of diabetes Exostosis occurs on the site of stress: Head of fifth metatarsal Distal talus Dorsal aspect of 1st metatarsophalangeal joint. It is the distal extremity of penis It accommodates a vertical slit like construction (opening)-called urethral meatus. A fold of skin extends from external urethral meatus to the prepuce-it is recognized as frenulum. Anteriorly they converge in entrance of vaginal orifice, every cut up into two folds that meet in the midline. Vestibule: It is a easy triangular space bounded: Laterally by labia minora Clitoris at its apex Fourchette at its base. It secretes acidic fluid-containing citric acid and acid phosphatase-which is added to seminal vesicles fluid on the time of ejaculation. Blood provide: Artery-interior vesicle and center rectal arteries Vein-prostatic venous plexus. Infundibulum: Funnel-shaped lateral end, fimbriated, fimbriae draped over the ovary. Cervix: Narrowest a half of uterus-divided into: � Supravaginal half � Vaginal half. Cavity in cervix is called cervical canal-it communicates: With the physique through inside os With vagina via external os. Uterus coated with peritoneum reflects: Anteriorly on to the bladder Posteriorly on to the rectum-producing a pouch-pouch of Douglas. Any history of earlier sexual contact current, is it oral, vaginal or anal contact If Number of sexual partners. Gonorrhea in men starts with dysuria and urethral discharge- 2�10 days after exposure. In woman-dysuria and vaginal discharge happen days to weeks after exposure-50 percent girls turn into asymptomatic. Penile lesion: History of penile lesions could also be suggestive of: Gonorrhea Syphilis Herpes Trichomoniasis Genitalia 1403 Venereal wart Other sexually transmitted disease. The rashes of genitalia are: Psoriasis: Most frequent, bright purple, well-defined, scaling plaques. Fixed drug eruptions: It is characterised by a quantity of, macular, eczematous, bullous patches. Lichen planus: Violaceous flat topped papules at the glans penis-Oral mucosa reveals white streaks on buccal mucosa. Causes of genital skin lumps: Most common: � Molluscum contagiosum � Coronal papillae in males � Vulval papillae in girls � Skin tags. Occasional: � Condyloma lata � Bowenoid papulosis-prostatic intraepithelial neoplasia. Scrotal enlargement: Questions to be requested: there any enlargement-for what quantity of days Is 1404 Clinical Methods and Interpretation in Medicine it recurrent-if so, how many occasions Erectile dysfunction: Persistent inability to achieve and preserve penile erection for enough time for passable sexual function: Causes: Physiological: � More than 50 years, married � Long-term monogamous relationship. Vascular causes: � Atherosclerotic stenosis of cavernous arteries � Vascular drawback related to smoking. Neurological cause: � Multiple sclerosis � Spinal wire tumor � Degenerative illness of spinal cord � Local nerve injury. Whether his associate is happy along with his sexual function, if not, why When was the final time he had satisfactory ejaculation During sexual activity, how long he is in a position to maintain his erection after penetration into vagina Constant use of condom-patient usually reports that condom split or come off during sex. To evaluate the purpose for infertility following histories to be taken: z Mumps z Injury to testes z History of publicity z Diabetes z Varicocele z Hypertension z Exposure to X-ray z Any surgical procedure Diabetic man may be infertile due to-retrograde ejaculation z Alcohol abuse z History of consumption of drugs z Sleeping habits z Type of labor he makes use of to carry out. Phimosis Narrowed opening at the prepuce due to incapability to retract the foreskin over the glans penis. Genitalia 1407 z Acquired: Infection-Balanoposthitis-Chronic Too forceful retraction of fore skin over the glans Adhesions as a outcome of poor hygiene. Sequelae If unrelieved, it may possibly trigger: z Urinary tract obstruction z Venous engorgement z Edema z Necrosis of pores and skin. Causes of paraphimosis z Too forceful retraction of foreskin over glans z Poor hygiene z Catheterization z Infection chronic balanoposthitis z Vigorous sexual activity. Lesion Moist macular lesion with yellow to black discoloration, having irregular borders and lichenification-due to papilloma virus an infection, finally resulting in phimosis. Causes: z Bacteria (Staphylococcus, Gardnerella, Streptococcus pyogenes) z Candida infection z Contact dermatitis. Balanitis In uncircumcised men in poor hygienic condition, accumulation of smegma produces irritation, edema and inflammation of glans- called balanitis. Predisposing components z Diabetes z Obesity z Old age z Edema z Contact dermatitis z Seborrheic dermatitis. Caused by: z Sexually transmitted organisms (Chlamydia, genital mycoplasma, gonococci). It will begin as painless bleb, in the end merging into giant ring of inflammatory lesion-completely circumscribing glans. Over palms and ft, lesion may be pustular and scaly resembling psoriasis (keratoderma blennorrhagica). Nonulcerating lesion: It is divided into: Papules <1 cm in diameter, raised above floor. Penile lesion in granuloma inguinale z Single, painless ulcer-friable, occurs in anogenital area or hypertrophic lesion-automatically resolved or slowly spread with tissue distraction. Penile ulcers in secondary syphilis z Multiple, painless, shallow irregular, grey ulcer involving penis- serpiginous ulcers. Penile lesion in herpes simplex Small, a number of, vesicular, painful ulcers arranged in clusters, because of herpes simplex type I virus. Penile lesion in pemphigus Fragile thin walled blisters-which break all the means down to painful or itchy ulcer in penis. Sebaceous glands: Small yellowish nodules, symmetrically distributed in ventral floor of shaft either seen or palpated as lump. Pearly penile papules: Multiple pearly coloured papules current around circumference of glans crown. Lichen sclerosus: It is described as atrophic white plaques seen in glans, foreskin or shaft as a result of persistent inflammation-it is asymptomatic. Its severe type is balanitis xerotica obliterans-in this situation, affirm, whitish, scarred appearance seen in uncircumcised prepuce. In this case, affected person is regular at relaxation, however throughout erection, the penis turns into bent, deformed and painful. Scrotal swelling: May be: z Bilateral: Diffuse, painless, edema, related to: Congestive cardiac failure Nephrotic syndrome Cirrhosis. In standing place, this engorged vein appears as nest of worms, but in supine place it is going to be resolved. Method of Testicular Palpation Prerequisite for palpation z Room should be sufficiently worm in order that the scrotal muscles contract to push the testes in course of inguinal canal. It incorporates: Vas deferens Testicular artery and vein Ilioinguinal nerve Lymphatic vessels Fatty tissue. Any lumpy feeling in spermatic cord might indicate varicocele because varicocele may be palpated in testes and spermatic wire. Hydrocele It is assortment of serum fluid both in tunica vaginalis or in separate pocket in spermatic cord. Spermatocele It is sperm stuffed cyst, nontender, unilateral cellular scrotal mass present above testes. Large testes It is usually testicular tumor or fluid filled testes-can be differentiated by transillumination take a look at. Inform the patient that you wish to examine anal canal and interior by inserting the fingers. Ask the affected person to bear down as if he was having a bowel motion and on the identical time, insert your finger into the anal canal easily due to leisure of anal sphincter. Genital Symptoms Female Questions to be asked: z Detailing of sexual partner and forms of sexual actions ought to direct the doctor to perform proper investigations and swabbing. Whether bleeding happens in between the period Whether she use contraceptive tablets. If Any change in vision Whether the patient is illiberal to warmth or cold there presence of any headache, nausea. Is Amenorrhea: Absence of menstrual bleeding: Primary: z Prepuberty z Menopause z Pregnancy. Secondary dysmenorrhea: If may happen because of: z Uterus: Intrauterine gadgets Uterine fibroid or polyp. Genitalia 1423 Mass or Lesions Questions to be requested: z When the lesion first occurred The following lesion, could also be present: z Chancre-painless nodule sharply demarcated border. Vaginal Discharge Questions to be asked z Whether any discharge is present or not. If may be due to: z Vulval soreness, vulval ulcer during early part of penetration z Lower belly pain in pelvic inflammatory disease, pelvic endometriosis during deep penetration. Bleeding per Vagina It may be because of: z Menstruation z Penetration into vagina z Gonococcal cervicitis z Vaginal ulcer z Chlamydia infection. Chronic belly pain could additionally be due to: z Ectopic endometrial tissue z Pelvic inflammatory illness of fallopian tube, ovaries z Pelvic muscle contraction as a result of protrusion of bladder, rectum, uterus.
Discount 80 mg top avana with mastercard. Ed Quits Smoking -- Day 5.