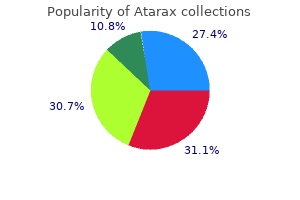
Aortic pressure is generated in a pulsatile method unrelated to left ventricular stress anxiety symptoms 89 buy generic atarax 10mg on line. Note the correspondence of pressures of the left and proper ventricles in most beats anxiety vs stress atarax 10mg on-line. Reduced left ventricular strain occurs when the timing of pump filling (b) (a) exceeds the timing of the native left ventricular ejection anxiety symptoms zinc order atarax 10 mg amex, and thereby ends in the alteration of left ventricular pressures anxiety symptoms 3 days discount 10 mg atarax otc. To assess the etiology of cardiac dysfunction anxiety symptoms teenager buy atarax 25 mg online, coronary angiography was performed and confirmed total occlusion of the left anterior descending anxiety pain buy discount atarax line, right coronary, and circumflex arteries. The single saphenous vein graft to the right coronary artery had a 50% ostial narrowing with mid graft 90% lesion. In the decrease proper nook is a continuous sign of pulmonary artery oxygen saturation, exhibiting a decline at peak train from 78% to approximately 40%. Exercise increased the assisted coronary heart fee (103 to 113 beats/min), mean arterial pressure (99 to 128 mm Hg), aortic diastolic stress (88 to one hundred fifteen mm Hg), left ventricular enddiastolic pressure (18 to 25 mm Hg), and pulmonary artery strain (45/15 to 75/28 mm Hg). Cardiac output (by thermodilution and confirmed by the console values) rose minimally (5. Coronary blood circulate (great cardiac vein) elevated (43 to fifty six min) with solely modest lactate technology. Consider the hemodynamic outcomes of exercise on this affected person with a left ventricular assist system with regard to train responses in normal subjects. Exercise normally increases heart price by greater than 25%, decreases aortic diastolic pressure due to decreased systemic vascular resistance, minimally modifications right ventricular and pulmonary artery pressures, and markedly will increase cardiac output and coronary blood circulate at least fourfold. In our affected person, the blunted heart rate and the rise in diastolic aortic and mean systemic pressures indicate a failure to lower systemic vascular resistance ortaaale arrroosallonarry ryoass 389 Table 21. The decline in pulmonary artery oxygen saturation is a markedly exaggerated response compared to a normal subject. The improve in pulmonary artery pressures also required explanation, with a left ventricular pump which is presumed to be substituting for native left ventricular work. The limited capability of the help pump to empty the native left ventricle results in elevated left ventricular enddiastolic stress and in addition pulmonary pressures. As one may anticipate, limited coronary blood flow by way of this severely diseased heart might be as a end result of arterial conduit blockage, as nicely as attenuated oxygen demand, with myocardial muscle performance supplemented by mechanical help. We speculate that the marked increase in pulmonary pressures reflects ischemia from the inferior left ventricular and right ventricular functioning zones. Right ventricular ischemia in the unassisted right ventricle would possibly nicely be the cause of progressive dyspnea, with compromised perform of the remaining lively myocardium of the inferior and lateral walls. Progression of coronary artery disease in the right coronary artery bypass graft (the solely remaining arterial blood supply) was evident. Limited blood move to the inferior left ventricular distribution more than likely affected the pressure responses to exercise. Several issues regarding alteration of left and proper ventricular chamber dimensions, mitral and tricuspid regurgitation, and left ventricular ischemic dysfunction require mixed echocardiographic imaging. This unusual hemodynamic case is illustrative of both the insights and limitations of hemodynamic data interpretation. In situations where complex questions of physiology are anticipated, explanations may be obtained with mixed echocardiographic and hemodynamic techniques. This kind of pump is generally related to decreased myocardial oxygen demand and is, at times, considered to "rest" the guts [10, 11]. Cardiopulmonary bypass has been used as an emergency "extra coronary heart" to assist circulatory collapse after acute myocardial infarction or cardiac arrest in the catheterization laboratory throughout diagnostic or therapeutic intervention [12�15]. Blood Pressure with a Closed Aortic Valve A 34yearold lady had extreme crushing chest ache with electrocardiographic proof of intensive anterior and lateral myocardial infarctions. A pulmonary artery balloon flotation catheter could be seen traversing the inferior vena cava. Twelve hours after admission to a community hospital, hypotension and ventricular tachyarrhythmias occurred. Initial resuscitative efforts had been profitable, with subsequent intubation and placement of femoral arterial and venous sheaths. Intravenous infusions of dopamine, lidocaine, and bretylium had been required to preserve a systolic blood strain of 80 mm Hg and secure sinus tachycardia. One hour after initial resuscitation and stabilization, hypotension and ventricular arrhythmias recurred. The affected person was transferred to the cardiac catheterization laboratory for diagnostic examine and potential angioplasty. Left ventricular operate was assessed before the cardiovascular surgeon would consider emergency coronary artery bypass grafting. Continuous pressure recording throughout left ventricular�aortic catheter pullback is shown at the proper aspect of the tracing after beat #4. The phasic character of left ventricular strain rapidly changes to a imply strain of the cardiopulmonary bypass circuit when the catheter is pulled throughout the aortic valve. These phasic waves reflect the left ventricular stress opening the aortic valve. During cardiopulmonary bypass, the left ventricle is contracting towards a closed aortic valve with no technique of left ventricular decompression. Left ventricular strain and wan stress are certainly elevated, as is myocardial oxygen demand. However, aortic stress is maintained sufficiently to perfuse the cerebral, renal, and coronary circulations. The crucial nature of cardiopulmonary bypass�augmented coronary perfusion was also demonstrated shortly after turning down the cardiopulmonary bypass system, reducing the mean blood stress to below 60 mm Hg. Aortic pressure is 55/40 mm Hg and proper atrial stress is sixteen mm Hg (0�40 mm Hg scale). With rising cardiopulmonary bypass circulate and restoration of an adequate systemic strain, the phasic aortic stress is obliterated and the best atrial stress falls as inferior vena caval blood is returned to the cardiopulmonary bypass circuit. With maintenance of coronary perfusion stress, the rhythm was converted right into a sinus tachycardia. Because of the important need to assess myocardial perform more than 18 hours after close to whole occlusion of the left coronary artery, a 15 cc distinction injection (low osmolar media, 15 cc/sec) was made into the left ventricle. The contraction pattern and regions of potential viability had been measured utilizing a digital angiographic approach. It is essential to cut back the cardiopulmonary bypass circulate to permit aortic valve opening throughout ventriculography for a sensible assessment of left ventricular contraction. Left ventricular pressure demonstrated a slow enhance in stress era and irregular strain decline during diastole. After beat #17, the catheter was pulled into the aorta and the mean systemic pressure of the moveable cardiopulmonary bypass could be observed. As flow rate is elevated, the aortic strain increases to a imply of 85 mm Hg and right atrial pressure falls from sixteen to 10 mm Hg. A choice for emergency coronary angioplasty was made after consultation with the cardiothoracic surgeon. The affected person expired 36 hours later because of acidosis, hypoxia, and renal failure. Extra hearts of the cardiopulmonary bypass selection with out ventricular decompression can preserve systemic perfusion, however accomplish that at the price of elevated myocardial work. Systemic pressure help facilitates emergency resuscitation and ought to be employed briefly till revascularization can be carried out. The hemodynamic waveforms in this affected person illustrate the paradox of systemic perfusion with increased myocardial ischemia. Without restoration of coronary perfusion, myocardial salvage, and ultimately survival, is very unlikely. An excellent evaluate of the physiologic basis for left ventricular assist devices is provided by Naidu et al. Those patients with the best danger and normally the bottom cardiac reserve were candidates for the most powerful assist. Additional profit is provided via the modification of the oxygen provide and demand steadiness, improving myocardial ischemia. Devices that may favorably alter the enddiastolic and endsystolic pressure�volume relationships can decrease myocardial work and supply myocardial protection from ischemia simultaneous with increased myocardial perform. Balloon deflation on the onset of systole decreases ventricular afterload and hence myocardial oxygen consumption (demand). The system consists of a single pigtail 12F catheter with inflow positioned in the left ventricle, outflow in the ascending aorta, and an included intravascular axial pump (maximal rotation 51,000 rotations per minute) that may deliver up to 2. The microaxial Archimedes impeller attracts blood from the left ventricle by way of an influx cannula and delivers nonpulsatile blood flow up to 2. Peripheral vascular illness and aortic valve illness are contraindications to the use of the Impella system. Increased aortic flow and stress improve flow velocity and decrease coronary microvascular resistance. The Impella has also been shown to instantly enhance overall hemodynamics in cardiogenic shock [25], including cardiac energy output [9] and endorgan microcirculation [26]; both outcomes appear to be favorable predictors of 30day outcomes in acute myocardial infarction with shock [27]. The Tandem Heart entails the placement of a 21 F catheter inserted into the left atria from the femoral vein via a transseptal puncture [28]. Blood is withdrawn from the left atrium by an exterior centrifugal pump and infused into the femoral artery by way of a 15�17 F catheter. Because of the big catheter diameter, iliacfemoral angiography must be performed previous to cannula insertion. The bluetagged cannula draws blood from the left atrium to the pump, which returns it to the femoral artery cannula. Nonetheless, on account of the unloading mechanisms, the Impella and Tandem Heart have the greatest influence on cardiac perform and hemodynamic stabilization. Key Points 1) Heterotopic heart transplant, while now out of date, demonstrates a few of the most attention-grabbing and distinctive hemodynamics exhibiting the affect of synchronous and dysynchronous systolic contraction of the donor heart. Experience with the Pierce�Donachy ventricular help gadget in postcardiotomy sufferers with cardiogenic shock. Myocardial oxygen consumption: Comparison between left atrial pulsatile synchronous and asynchronous bypass. Diastolic balloon pumping (with carbon dioxide) in the aorta: A mechanical help to the failing circulation. Improved hemodynamic and left ventricular unloading during acute ischemia utilizing the left ventricular assist device compared to intraaortic balloon counterpulsation. Percutaneous left 12 13 14 15 16 17 18 19 20 21 atrial femoral artery bypass with a pulsatile pump: Initial experience in cardiogenic shock. Initial report of the National Registry of Elective Cardiopulmonary Bypass Supported Coronary Angioplasty. Percutaneous cardiopulmonary bypass assist within the catheterization laboratory: Technique and issues. Novel percutaneous cardiac assist devices: the science of and indications for hemodynamic help. Cardiac energy output predicts mortality throughout a broad spectrum of patients with acute cardiac disease. Hemodynamic variables and mortality in cardiogenic shock: A retrospective cohort study. Elective intraaortic balloon counterpulsation during highrisk percutaneous coronary intervention: A randomized controlled trial. Augmentation of coronary blood move by intraaortic balloon pumping in sufferers after coronary angioplasty. Miniature intracardiac help device provides more practical cardiac unloading and circulatory support during severe left heart failure than intraaortic balloon pumping. Seyfarth M, Sibbing D, Bauer I, Fr�hlich G, BottFl�gel L, Byrne R, Dirschinger J, et al. A randomized clinical trial to consider the safety and efficacy of a percutaneous left ventricular assist system versus intra aortic balloon pumping for remedy of cardiogenic shock caused by myocardial infarction. Effects of mechanical left ventricular unloading by Impella on left ventricular dynamics in highrisk and primary percutaneous coronary intervention patients. The Tandem Heart, percutaneous transseptal left ventricular assist device: A safeguard in highrisk percutaneous coronary interventions: the sixyear Rotterdam expertise. Randomized comparability of intraaortic balloon help with a percutaneous left ventricular help gadget in patients with revascularized acute myocardial infarction difficult by cardiogenic shock. Rapid identification of the mechanisms contributing to hemodynamic compromise is important because (i) if not treated expeditiously, shock typically leads to demise; (ii) its management varies relying on the trigger; and (iii) management for one etiology could additionally be deleterious for another. Shock evaluation is predicated on the 2 keys of building the etiology and assessing the hemodynamic status, processes which proceed concurrently and instantly: 1) Hemodynamic evaluation: Immediate bedside evaluation of hemodynamic status serves as the muse of emergency administration. Hemodynamic classification may be additional refined by invasive assessment with rightheart catheterization. Cardiogenic shock is defined as systemic tissue hypoperfusion secondary to insufficient cardiac output regardless of enough circulatory quantity and ventricular filling strain. However, further evaluation is usually essential, together with urgent noninvasive evaluation. The following circumstances illustrate principles of evaluation and methods for management of advanced cardiogenic shock. Intravascular ultrasound revealed delicate dissection on the distal stent edge, which was handled with an overlapping drugeluting stent. Repeat intravascular ultrasound revealed a wellexpanded and wellapposed stent ase # 403 Table 22. Following coronary intervention, additional hemodynamic measurements were obtained (Table 22. The affected person was transferred to the operating room, where the best axially artery was exposed by surgical cutdown.
Cough increases both aortic stress (>240 mm Hg) and proper atrial stress (210 mm Hg) anxiety symptoms body zaps order atarax with american express, together producing a marked and parallel pressure enhance anxiety guru purchase cheap atarax. As the atrial contribution returns to the rhythm anxiety ocd order atarax 25 mg without a prescription, circulate velocity undergoes solely an insignificant change anxiety symptoms last for days order atarax 25mg. Although lack of atrial activity with decreased aortic pressure would likely scale back demand anxiety symptoms journal order atarax in india, the outcome on autoregulation in this affected person was not reflected in a discount in coronary circulate velocity anxiety 2020 episodes cheap atarax 10 mg line. Coronary Flow Velocity throughout Atrial Fibrillation Atrial fibrillation is a typical arrhythmia during which very fast ventricular depolarizations might cause ineffective arterial stress generation. Although a lack of coronary flow in the course of the pulse deficit might be anticipated, coronary flow velocity has not been commonly observed in these sufferers. Coronary blood flow in beat #4 was abbreviated by the following early ventricular beat (flow integral = 5. The move velocity was maintained in the course of the subsequent rapid beats regardless of the loss of arterial stress. A small arterial stress wave, generated by beat #5, was related to important augmentation of the coronary blood circulate integral (20. Coronary Flow throughout Ventricular Tachycardia Although rarely witnessed, as one would possibly expect, coronary blood flow ceases through the disorganized rhythm of ventricular tachycardia. Ineffective ventricular systole limits stress technology and the markedly shortened diastole fails to allow ventricular rest, curtailing coronary flow. Coronary flow velocity was measured in a affected person undergoing diagnostic catheterization to determine coronary vasodilatory reserve. Intracoronary papaverine (10 mg) was used because the hyperemic stimulus to produce maximal coronary flow. The cough pulse strain (B) is related to a marked decrease in coronary circulate velocity without any augmentation of both peak or mean flow on the subsequent beat(s). The limited and infrequently decreased flow velocity is current whether single or multiple coughs are performed. Benign sinus arrhythmia and regular respiratory activity trigger cyclical alterations in aortic strain. Small modifications in myocardial oxygen demand occur, according to the growing and decreasing coronary heart rate�pressure merchandise. The mean and peak phasic circulate velocity indicators show parallel adjustments in response to alteration in arterial strain during respiration. Coronary move velocity, as shown in this patient, precisely displays the autoregulatory response of the traditional coronary circulation. With the appreciation of autoregulation and its impact on coronary circulate velocity, can one predict what the result of loss of atrial exercise would do to coronary move velocity Aortic stress and imply and phasic coronary move velocity had been measured throughout a period of transition from sinus rhythm to paced rhythm and return to sinus rhythm. These effects on coronary circulate are current whether or not coronary move velocity is measured proximally (top tracings of panels) or distally (bottom tracings of panels). During ventricular tachycardia, when aortic stress was not produced, coronary blood move velocity quickly fell to zero. Immediate defibrillation restored both rhythm and coronary flow, with no residual antagonistic effects. Regardless of the coronary circulate patterns, restoration of a traditional rhythm for these patients is of apparent significance. Note the marked decline in arterial strain (c, first arrow) with return on the following respiratory cycle (second arrow). Recent advances in Doppler methodologies permit straightforward measurement of coronary blood circulate during routine coronary angiography. At the present time, measurement of coronary blood circulate velocity remains principally a research approach, but is of continuing interest in medical syndromes of atypical angina, myocardial hypertrophy and infarction, early transplant rejection, or premature (subangiographic) atherosclerosis in some patients. First, coronary reserve may be calculated because the ratio of imply Coronary loow eserre anddHyperemia 335 hyperemic to basal coronary move velocity. Normal coronary vasodilatory reserve has been reported as a variety depending on the scientific characteristics, but higher than 3. Coronary hyperemic responses could also be altered by metabolic, vascular, myocardial, and endothelial factors [59], and additional concerns beyond the scope of this dialogue. Coronary hyperemia is outlined as a transient or everlasting increase in coronary flow above the basal stage in response to train, pharmacologic stimulation, or reduction of ischemia. Reactive hyperemia describes the coronary move response occurring after relief of transient arterial occlusion, producing ischemia. In sufferers, reactive hyperemia may be produced following balloon deflation during coronary angioplasty. Coronary vasodilatory reserve, the ratio of basal to maximal hyperemic move, is taken into account to be the maximal increase in circulate that could be achieved by the stimulated 2 sec coronary bed. Although measurements of coronary hyperemia and coronary reserve may be simply obtained within the cardiac catheterization laboratory with coronary Doppler strategies, the appliance of this technique presently remains principally for research. There are two strategies obtainable for measuring coronary blood flow reserve within the catheterization laboratory: intracoronary Doppler circulate velocity and coronary artery thermodilution. Coronary Doppler Flow Velocity Unlike the strain wire, measuring move velocity with the Doppler sensor wire requires no zeroing or central sign matching. Once sensor connections and the rate settings on the display screen show are set, the Doppler wire is handed past the stenosis with the Doppler guidewire tip positioned a minimum of 5�10 arterydiameter lengths (>2 cm) past the goal stenosis. Because of the extremely positiondependent sign, poor signal acquisition could happen in 10�15% of sufferers even within regular arteries. As with transthoracic echo Doppler studies, the operator should regulate the guidewire place (sample volume) to optimize the velocity sign. Influence of Hemodynamics on Coronary Flow Reserve Guidewire Thermodilution Blood Flow Technique the coronary thermodilution approach uses thermistors on a pressuresensor angioplasty guidewire and measures the arrival time of roomtemperature saline bolus indicator injections by way of the guiding catheter into the coronary artery [64, 65]. When mixed with stress measurements, coronary flow reserve measurements can present a complete description of the pressure�flow relationship and the response of the microcirculation. Pharmacologic Agents for Coronary Hyperemia Stenosis severity should at all times be assessed utilizing measurements obtained during maximal hyperemia. The most generally used maximal vasodilator agent for dedication of coronary vasodilatory reserve is adenosine. Nitrates enhance volumetric circulate, but, because these brokers also dilate epicardial conductance vessels, the increase in coronary circulate velocity is less than with adenosine or papaverine. Increasing imply arterial strain reduces maximal vasodilation, decreasing hyperemia with much less alteration in basal move. Patients receiving methylxanthines or similar medication might have a markedly lowered impact from dipyridamole. Side results from dipyridamole, together with flushing, chest ache, and nausea, are quickly reversed by theophylline administration. Doses above 200 mcg are related to significant decreases in imply arterial strain and fall in coronary hyperemia. Nitroglycerininduced hyperemic effects occur inside 20 � 5 sec, with a length of up to 90�110 sec. Sodium nitroprusside additionally appears to be a suitable hyperemic stimulus for coronary physiological measurements. Maximal hyperemia occurs 28 � 15 sec after intracoronary injection and returns to baseline inside 128 � 15 sec [66]. Since low doses of papaverine could not elicit maximal hyperemia, an initial dose of 8�10 mg is administered, with a second 12 mg dose to affirm a maximal vasodilatory response. Regadenoson is an 2A adenosine receptor agonist that induces coronary vasodilatation and will increase myocardial blood flow in a fashion reportedly equal to adenosine, with fewer opposed effects. Regadenoson has a halflife of 2�3 min in the initial section, 30 min in the intermediate section, and a pair of hours within the terminal part. Coronary Hemodynamic Tracings within the Catheterization Laboratory 341 Coronary Hemodynamic Tracings within the Catheterization Laboratory: Catheter Tip Pressures Observing the arterial pressure waveform from the tip of the catheter during coronary angiography is an important key to a safe process [77�79]. One of the earliest clues to the presence of left major coronary stenosis is a characteristically abnormal arterial pressure instantly upon catheter engagement of the coronary ostium. The pressure waves in these patients are sometimes referred to as ventricularized or damped. Ventricularization or damping of coronary arterial strain has a recognized association with left major coronary stenosis by skilled angiographers over a number of many years [80, 81]. Cases: Pressure Ventricularization A 60yearold girl had a oneyear history of exertional chest pain, with progressive ache over the previous three months. In the past month, episodes of chest ache had occurred with minimal exertion and at relaxation. The patient was admitted to the hospital and scheduled for cardiac catheterization the next day. On catheter tip engagement, arterial pressure dropped from 140 to 60 mm Hg (systolic), with diastolic pressures dropping from 80 to 35 mm Hg. A transient coronary injection was carried out with immediate withdrawal of the catheter, as evidenced by the fast return of arterial strain to normal. Note the wide pulse stress, speedy diastolic decline, and small constructive deflection immediately before systolic upstroke. To restrict the time of impaired perfusion with the catheter partially obstructing the coronary ostium, the operator carried out a "hitandrun" maneuver with brief contrast injection and rapid elimination of the catheter. A comparable hemodynamic tracing was obtained in a 65 yearold man with chest ache following coronary artery bypass graft surgery. Coronary arteriography was carried out with immediate withdrawal of the catheter tip ("hitandrun" maneuver). On engagement of the left main coronary artery, ventricularization of the strain waveform is noted. Contrast injection happens during a brief "hitandrun" interval lasting approximately 5�7 sec after withdrawal of the catheter. Note the alterations of electrocardiogram immediately after distinction injection with marked T wave inversion. Pressure Damping Significant strain adjustments occurring when a coronary catheter tip obstructs artery move into a flattening of the strain wave are known as "damping. In general, right coronary waveform strain alterations are more widespread, due, in part, to a smaller artery, subselective conus branch engagement, or catheterinduced coronary spasm. These changes carry less significant consequences except left major or extreme multivessel left coronary stenoses are additionally current. Thallium scintigraphic redistribution was present within the inferior and lateral regions. The injector syringe strain was recorded, demonstrating the time, duration, and depth (pressure) of hand injection during the proper coronary artery angiogram. The hitandrun maneuver additionally exhibits the instant return of normal arterial strain upon completion of catheter withdrawal during contrast injection. The technique of contrast injection is demonstrated by the injection syringe strain (arrow), which was measured during this examine. There had been no important electrocardiographic abnormalities during this injection. From examination of the two pressures, the coronary pressure was really left ventricular pressure. This catheter had slipped into the left ventricle and, previous to distinction injection, asystole occurred, in all probability by stimulation of the left bundle creating transient left bundle block in the setting of a preexisting proper bundle branch block. On catheter removal, restoration of the left bundle conduction occurred and cardiac rhythm was restored with regular blood stress. The morphology of ventricularized coronary stress additionally has a definite presystolic deflection, resembling an "a" wave. The upstroke is also slower than aortic stress and the downstroke steeper than aortic stress. However, an inattentive operator might take a number of seconds to react promptly to restrict asystole and hypotension. Mechanisms of Ventricularization the mechanisms of coronary strain damping have been studied by Pacold et al. Variable levels of intracoronary strain modifications upon cannulation of diseased left primary coronary arteries have been observed in 20 consecutive sufferers with ventricularization of coronary strain. Confirmation of those stress waveforms was obtained in an animal model by inserting a balloon tipped catheter and producing partial levels of occlusion of the left major coronary artery. The ventricularized pressure wave is derived from aortic stress, which is altered by its transmission throughout the narrowed left major coronary artery. Advancing a catheter into the ostium of a narrowed coronary artery reduces each systolic and diastolic pressures, as properly as inflicting a steep decline of the pressure in diastole. A attribute increase in pressure at enddiastole with a presystolic optimistic deflection was thought to be related to atrial contraction. The degree of pressure drop between the ascending aorta and a stenosed left major coronary artery is variable, depending on the degree of stenosis. Pressures from small proper coronary arteries and stenosed proximal vein grafts can also reveal this phenomenon. Ventricularization stays a crucial remark related to left primary coronary artery stenosis. Appropriate particular strategies to acquire secure angiograms for this situation should be employed [81]. A lowvolume, digital subtraction ventriculogram may be a helpful "onetest" study for quick surgical session. In patients with crucial left main stenosis, insertion of an intraaortic balloon pump and speedy switch for emergency cardiac surgery could also be required. Pressure Damping Due to Catheter Tip Abutment against the Arterial Wall Pressure damping due to true left major stenosis must be differentiated from damping due to the tip of the catheter set flush towards the vessel wall. Catheter withdrawal, repositioning, reangulation, and cusp injection ought to be carried out. Patient management will differ according to the laboratory experience and coaching of the operators. Recognition and appreciation of abnormal coronary pressure waveforms could directly have an effect on the life and dying of these sufferers. Key Points 1) Measurements of coronary strain and move in the catheterization laboratory at the second are used in day by day clinical practice and related to improved scientific outcomes for percutaneous coronary intervention decisionmaking.
A 19-year-old man with autism and extreme hemophilia B is thought to have developed an inhibitor anxiety wikipedia generic 25mg atarax. She is currently within the preoperative holding area acute anxiety 5 letters atarax 10 mg, and hematology is urgently consulted anxiety 6 months postpartum buy discount atarax online. She has undergone a right complete knee replacement with this orthopedic surgeon in the past with good outcomes anxiety lexapro side effects atarax 10 mg with amex, prompting her to have the left knee replaced anxiety uk order 25mg atarax fast delivery. Four-factor prothrombin complex concentrate anxiety yellow pill atarax 25mg amex, 2500 units half-hour prior to surgical procedure 252 Coagulation fifty nine. However, she suddenly developed a severe headache with photophobia and meningeal indicators. A 21-year-old college student presents to the University Student Health Care Center with a several-year history of heavy menstrual bleeding. She has had an extended history of intermittent epistaxis however in any other case no major bleeding or bruising. A session is requested for a patient is a 54-year-old homeless man, with a previous history of schizophrenia and alcohol abuse. He was discovered unresponsive in the center of a sidewalk and was initially thought to be the sufferer of assault. This prompted a closer physical examination and revealed the looks of "petechiae" along his hair follicles, in addition to gingival swelling, main the medical student to suspect leukemic infiltration. A session is urgently called to evaluate a 74-year-old man on the orthopedic service. His past medical historical past is outstanding for hypertension, diabetes mellitus, nonischemic cardiomyopathy, and atrial fibrillation, for which he has been maintained on therapeutic anticoagulation with warfarin. He had been admitted for an elective right total hip arthroplasty, following which he resumed anticoagulation with warfarin at his residence dose. Prior to his discharge to rehabilitation, he developed a fever and was famous to have erythema of the surgical website. He was started on piperacillin/tazobactam and gentamicin, but the following day purulent discharge was famous to be coming from the wound. A 14-year-old lady recently offered to her pediatrician for heavy menstrual bleeding. As a baby she experienced frequent bruising and a knee hemarthrosis after falling off her bicycle. A 25-year-old lady is referred for evaluation of epistaxis and straightforward bruising that she has had for a number of years. She can relay that she has had a protracted history of easy bruising, heavy menstrual cycles, and subcutaneous hematomas. As a toddler she had umbilical stump bleeding and one spontaneous intracranial hemorrhage. A 45-year-old male of Ashkenazi Jewish descent is shipped for perioperative recommendations prior to a deliberate total hip arthroplasty. He notes that he had extreme bleeding previously after a cholecystectomy, appendectomy, and after wisdom tooth extraction. She is scheduled to endure an belly hysterectomy for fibroid uterus subsequent week. A 42-year-old woman presents with a history of recurrent miscarriages and a bleeding disorder diagnosed at 254 Coagulation Which of the next most accurately describes the mechanism leading to this drug-induced thrombocytopenia He has only required two doses his complete life: once for circumcision and as quickly as for a knee hemarthrosis. Over the last 2 months he and his spouse have seen increased spontaneous joint bleeding with minor activity. An in any other case wholesome 18-year-old man presents with a swollen, tender knee 12 hours following trauma. A 79-year-old man with a history of hypertension and severe aortic stenosis (mean gradient >40 mm Hg) presents with melena. Approximately 8 hours later she develops epistaxis, hematuria, and bleeding at her central venous catheter website. Which of the next is probably the most appropriate treatment previous to his dental surgical procedure A 58-year-old man with a history of sort I von Willebrand illness plans to have two enamel extracted in 1 week. He has utilized epsilon aminocaproic acid (Amicar) following earlier dental extractions with sufficient control of bleeding. Which assertion greatest describes the mechanism of action of epsilon aminocaproic acid He bruises spontaneously and has skilled recurring epistaxis and gingival bleeding since delivery. His dad and mom indicate he experienced umbilical stump bleeding after detachment of the umbilical twine. Prothrombin time, partial thromboplastin time, and thrombin time are within normal limits. A 79-year-old man with a history of hypertension presents with new onset of severe left arm ache and swelling secondary to compartment syndrome from an intramuscular hematoma. He needs to proceed to the operating room for urgent fasciotomy because of the compartment syndrome. She has four full siblings, a sister who has skilled menorrhagia and three brothers, considered one of whom has had hemarthroses and delicate tissue bleeds. A 31-year-old G1P0 with severe kind 1 von Willebrand disease presents in lively labor at 38 weeks gestation while on trip to visit her household. She has been under the care of a high-risk obstetrician throughout her being pregnant and has not had any issues. A 68-year-old with type 1 von Willebrand disease presents with a latest diagnosis of nephrolithiasis after the onset of stomach pain and gross hematuria. He complains of two years of diarrhea and a 40-pound weight reduction and worsening dyspnea on exertion. He denies any history of abnormal bleeding, though he has noted simple bruising over the past 3 months. A bone marrow biopsy reveals 8% lambda-restricted plasma cells; Congo red staining is adverse for amyloid deposition. He has had two transient ischemic attacks within the last yr, has medication-controlled hypertension, and diabetes mellitus kind 2. He has gentle arthropathy involving the left knee and ankle, however in any other case no target joints. He has had only some bleeding episodes in his lifetime, every secondary to trauma. She awoke the next morning with a pillow soaked with blood and required packing and stitching. Her mother and two older sisters also have heavy menstrual bleeding, and her mother required a hysterectomy at age 26 for bleeding. A 55-year-old man with severe hemophilia A presents to the emergency department with headache and vomiting after falling and hitting his head on stone steps. The patient has regular important signs and is noted to have a big temporoparietal hematoma of his scalp. She has never had irregular bleeding together with her prior surgical procedures, together with cesarean part � 2, cholecystectomy, hysterectomy, and bilateral cataract extractions. Physical examination is critical for multiple ecchymoses over all extremities and the left flank. Which of the next measurements is the best way to follow the hemostatic efficacy of this remedy A 35-year-old lady presents for analysis of bleeding administration with upcoming surgery to appropriate a deviated nasal septum. She bled abnormally with wisdom tooth extraction requiring transfusion and has had a severe muscle hematoma following a snowboarding accident when she landed on an ice block along with her left thigh. She had heavy menstrual bleeding requiring oral contraceptive pills beginning at age 14. A 65-year-old man with extreme congestive coronary heart failure had a steady move left ventricular help gadget implanted four months ago. He has by no means had irregular bleeding before and actually had undergone a number of 258 Coagulation shows muffled coronary heart sounds, decreased breath sounds on the bases bilaterally, and ascites is present. Large bruises at all phases of therapeutic are present over the thighs, calves, shins, and buttocks. Bone marrow biopsy reveals 3% monoclonal plasma cells and pinkish materials, which provides apple green birefringence on Congo purple staining. A 33-year-old woman presents for evaluation of abnormal bleeding following sinus surgical procedure. She did nicely initially but then was famous to have significant bleeding later that afternoon, about 6 hours postoperatively. A 66-year-old man with atrial fibrillation for 20 years and gentle dementia for the previous 2 years is brought in by his daughter with multiple bruises on his extremities and epistaxis. The patient has been treated with dabigatran and atenolol, and has confused his medications. He has massive ecchymosis on his upper and lower extremities, brilliant pink surgeries and tooth extractions accomplished with out unusual bleeding earlier than implantation of his cardiac gadget. A 55-year-old lady with a historical past of smoldering myeloma presents with new onset severe bruising and hematoma formation. Which of the next laboratory test is most likely to lead to the correct diagnosis Past medical historical past is critical for degenerative joint illness, depression, and anxiety. Physical examination reveals an anxious, ill-appearing lady, struggling hematemesis and melena. She is handled with vitamin K and four-factor prothrombin advanced focus, with complete resolution of bleeding and correction of clotting instances over the course of 3 days. Which of the following diagnostic tests is more than likely to result in the correct diagnosis He has noted progressive ankle swelling and has developed elevated abdominal girth. A 65-year-old lady with a 20-year history of atrial fibrillation managed with dabigatran for the past 2 years presents with acute appendicitis necessitating surgical intervention. Her physical examination is exceptional for a temperature of 102�F, pulse of 110, and guarding and rebound in her left decrease quadrant. A 27-year-old girl presents with pain and swelling in her left leg 24 hours after beginning clomiphene for infertility. On additional analysis, she is found to be heterozygous for the prothrombin 20210 mutation. She was subsequently found to have a lupus anticoagulant and IgG anticardiolipin antibodies at a moderately optimistic titer (40), with antibodies to beta 2 glycoprotein1. Further evaluation revealed a serum homocysteine 259 stage of 15 m/L that was top normal for the laboratory during which it was tested. A 27-year-old woman at 33 weeks gestation presents to the emergency room with crampy abdominal ache and bleeding. The obstetrician suspects antiphospholipid antibody syndrome and begins the suitable laboratory evaluation. Which of the next laboratory research would assist the diagnosis of antiphospholipid antibody syndrome A 54-year-old lady with no prior medical historical past develops stomach ache and is discovered to have ascites. Screening was carried out within the offered affected person, and she or he is also found to be heterozygous for the prothrombin gene mutation (P20210). He wish to keep away from injectable medications and to be discharged as quickly as potential. He is presently on no drugs that would work together with warfarin or any of the new oral anticoagulants. He was in his usual state of good, having lately flown from Munich to Chicago, when he developed progressive right-sided pleuritic chest pain over the course of 2 days. Two sets of Troponin-I are unfavorable for cardiac harm, and he remains hemodynamically steady, requiring solely 2 L of supplemental oxygen through nasal cannula. At the same time, bilateral lower extremity ultrasound is carried out, showing occlusive thrombus from the left frequent femoral to popliteal vein, becoming nonocclusive within the trifurcation and extending into one of many paired tibial veins. A 58-year-old man has been sent for a consultation from the cardiovascular surgery clinic. This showed diffuse coronary artery disease that was not amenable to percutaneous intervention and extreme mitral stenosis. Following his process, the platelet depend was noticed to have dramatically declined to a nadir of 53,000 � 109/L. He was empirically positioned on a bivalirudin infusion and bridged to warfarin after his platelet rely remained larger than 150 for two days, which he remained upon since that time. While there have been no hemorrhagic complications from the use of his warfarin, he has developed progressive dyspnea on exertion and was sent to the cardiovascular surgical procedure clinic for an evaluation for mitral valve substitute. Given his comorbidities, it was not felt that he was an acceptable candidate for either a percutaneous or minimally invasive laparoscopic approach for repair of his valve. It was really helpful that he endure an open mitral valve replacement with a mechanical valve on bypass. Thomas has been despatched to the Hematology Clinic for suggestions concerning his use of warfarin and his prior publicity to heparin. She had been in her usual state of health, which was characterised by gastroesophageal reflux disease, weight problems, and tobacco use, when she developed proper calf pain and tenderness that progressed over the course of four days.
Purchase atarax amex. Simple Routine for Children's Separation Anxiety.