In such conditions blood pressure medication beginning with m order generic avalide, extension of the cervical backbone may cause neurological deficits as a outcome of it produces an opening wedge osteotomy in a normally kyphotic cervicothoracic spine blood pressure quiz pdf order 162.5 mg avalide fast delivery. A thorough historical past must be obtained from the patient prehypertension parameters buy cheap avalide 162.5mg on-line, if attainable arrhythmia frequently asked questions discount avalide 162.5mg with amex, or from family members or witnesses to the harm hypertension juice recipe generic avalide 162.5 mg with visa. A detailed history involving medical comorbidities blood pressure kits walmart purchase avalide without a prescription, prior surgeries, description of the injury, time of incidence, presence and location of ache, severity and outline of ache, neurological symptoms within the trunk and extremities (both transient or sustained), and prior spinal pathology is relevant to the administration of the patient. A dedication of underlying cardiopulmonary comorbidities together with persistent obstructive pulmonary disease and coronary heart illness is essential, especially within the setting of chest wall or lung damage. The physical examination begins with a visible inspection of the backbone for malalignment, swelling, bruising, lacerations, and different lesions. Palpation of the backbone from the skull to sacrum is performed for identifying tenderness, step-offs, gapped spinous processes, and different vital findings. Pain at the affected space is the most common presenting symptom after cervical trauma. An examination for other nonspinal musculoskeletal and nonorthopedic injuries is routinely accomplished as a part of a radical scientific evaluation. Early recognition of cervical backbone accidents by thorough history-taking, examination, and imaging might forestall neurological decline, enhance outcomes, and mitigate the chance of delayed prognosis and treatment, which occurs in practically 33% of cervical backbone sufferers. However, high-energy accidents with unilateral, a number of myotomal involvement may finish up from brachial plexopathy. The sensory examination consists of evaluation of light contact and pin prick and is categorized as absent (0), impaired (1), or normal (2). Myotomes in the extremities are graded as whole paralysis (0), palpable or seen contractions (1), movement with gravity eradicated (2), movement towards gravity only (3), movement towards gravity with some resistance (4), and regular energy (5). The assessment of sacral sensation on the perianal space and deep sensation with digital rectal examination is a crucial facet of the bodily examination due to its prognostic significance. Sacral sparing, which is the retention of sacral sensation, within the setting of absent motor indicates an incomplete injury. Sensory loss and bladder dysfunction are variable after traumatic central wire syndrome. Signs of an epidural hematoma embrace progression of ascending weak spot and weakness inside hours of an injury. An examination of upper extremity, lower extremity, and bulbocavernosus reflexes is critical. Initial flaccid paralysis, full lack of sensation, and absent reflexes after a traumatic damage is referred to as spinal shock. In the absence of spinal shock, reflexes in the extremities are useful for differentiating a nerve root harm from a cord injury. Altered reflexes occur in roughly 20% of injuries to the proximal cervical spine. The maneuver is carried out by pinching the glans penis (clitoris in females) or tugging the Foley catheter and monitoring for involuntary contraction of the anal sphincter. Cranial nerve perform might present extra information relating to the extent of harm. The incidence of cranial nerve dysfunction is low after occipitocervical trauma (3. Occipital condyle fractures, for example, might end in hypoglossal nerve dysfunction as a result of the hypoglossal canal is positioned medially and superiorly to the condyles. Occipitocervical fractures can cause harm to the brainstem in which the nuclei of cranial nerves three to eight are located. Injury to the medulla can produce dysfunction of cranial nerves nine through twelve. An analysis for a supply of hemorrhagic shock is warranted as a outcome of each hemorrhagic and neurogenic shock may be current. Autonomic dysfunction inhibits the conventional physiologic responses to blood loss: tachycardia and peripheral vasoconstriction. Patients could present with vertebrobasilar insufficiency (dizziness, ataxia, and vision changes), dysphagia, facial numbness, vertigo, Horner syndrome, or indicators of anterior spinal twine ischemia (complete motor paralysis, lack of pain and temperature, autonomic dysfunction, areflexia, urinary retention, and retained proprioception and vibratory sensation). Radiography, although much less sensitive and specific than the superior techniques, has traditionally been used for preliminary 28 Initial Assessment (Including Imaging) of Cervical Spinal Cord Injury imaging in awake patients. In addition, soft-tissue pathology and presence of a hematoma can be evaluated with using soft-tissue windows. Dynamic views have been advocated within the awake, cooperative, symptomatic patient with regular static X-rays to exclude discoligamentous injuries. The occipitocervical and subaxial backbone is assessed for occipitocervical damage, atlantoaxial fractures and instability, aspect dislocations, vertebral physique fractures, listhesis, and posttraumatic kyphosis, among different injuries. Radiographs can be utilized to determine atlanto-occipital dissociation; nonetheless, the sensitivity for identifying pathology is poor. Vertebral bodies should be analyzed for radiolucencies indicating fracture traces, peak loss, subluxation, side pathology, and angulation. Distraction of spinous processes on lateral radiographs signifies a hyperflexion mechanism. Soft-tissue harm anterior to the cervical spine is represented by prevertebral soft-tissue swelling, which is measured between the anterior floor of the vertebral our bodies and the air shadow of the airway. Various limits of normal have been reported from roughly 3 to 10 mm between C2 and C4. In addition to traumatic injuries, underlying degenerative changes and congenital stenosis of the cervical backbone are necessary to recognize because of their contribution to twine injuries, such as central cord syndrome. The morphology of the fractured lamina and left pedicle is well visualized, in addition to protrusion of bony fragments into the spinal canal. The condyle�C1 interval has the highest sensitivity and specificity for atlanto-occipital dissociation among all measurement parameters. Spinal twine compression towards the posterior cortex of C2 and a excessive fee of neurological injury42 occurs after these atypical fractures. In addition to delineating bony pathology, traumatic disc herniations and epidural hemorrhage may be recognized by delicate tissue and lung home windows. Flanders et al50 reported that craniocaudal length of edema and excessive cervical lesions correlated with poor functional outcomes. Sagittal T2-weighted photographs are crucial for the analysis of the spinal twine and are the one sequences which have prognostic worth, but axial photographs additionally provide detail about the amount of spinal wire compression, canal compromise, and site of disc herniation. T1-weighted photographs, in contrast, present wonderful delineation of anatomic constructions including the main ligaments of the spine. Spinal twine pathology may also be assessed on T1 imaging regardless of the normal use of T2 signal abnormalities for routine clinical assessment. Edema, hyperacute hemorrhage, and infarction appear darkish on T1-weighted imaging whereas subacute hemorrhage may be seen as a bright sign. Hemorrhage in the spinal wire is identified by hypointensity on T2-weighted imaging. Hemorrhage commonly happens within the nuclei of the spinal wire and represents the purpose of most influence. In the cervical backbone, intraspinal hemorrhage reflects a whole neurological injury. In the case of a bigger hemorrhage, more time is required for deoxyhemoglobin to be converted into methemoglobin. A thorough evaluation of anterior and posterior ligamentous constructions is crucial especially within the setting of vertebral subluxation or dislocation. The ligamentous anatomy of the upper cervical spine maintains spinal alignment and stability. The failure of all anterior structures or all posterior plus two anterior constructions is a threat factor for cervical instability. Posterior ligamentous advanced injuries can have an result on the supraspinous ligament, interspinous ligament, and ligamentum flavum. Ligamentum flavum harm can be seen as discontinuity or displacement into the thecal sac. Additional injuries were identified in 12% of sufferers, which included ligamentous injuries, fractures, and dislocations. Subluxation, transverse foramen fractures, and cervical accidents between C1 and C3 are probably the most generally cited risk components for arterial injury. In this study, intramural hematomas are seen on T1 imaging as a hyperintense rim surrounding a flow void. An enhance in arterial diameter compared to the contralateral artery is one other indicator of damage. Disadvantages, such as length of imaging time, undefined effectiveness of imaging extra body areas in the acutely injured affected person with this modality, and low specificity and sensitivity, restrict its use in the trauma setting. Marrow edema from trabecular microfractures indicates vertebral body fracture however edema is less likely to occur within the bony posterior elements. This imaging method measures velocity and directionality of water molecules along linear constructions, similar to nerve fibers, and identifies abnormalities of linear molecular motion. Fractional anisotropy is a generally referenced parameter that ranges from 0 (representing isotropic diffusion or movement in a sphere) to 1 (representing anisotropic diffusion in a cylinder). Fractional anisotropy normally approximates the value "1" because intact nerve fibers are long, thin cylinders. If an damage occurs, the diffusion of water molecules turns into unrestricted (isotropic) and approaches "0". Cervical fractures are sometimes secondary to hyperextension and are unstable, three-column injuries. As a result, the chance of neurological harm after cervical harm is 3 times larger than the overall population. In a evaluate of ankylosing spondylitis patients with cervical fractures, radiography when used alone was unable to visualize the complete cervical backbone in 92% of sufferers, and only 48% of fractures could possibly be recognized. Introduction to the guidelines for the management of acute cervical backbone and spinal cord accidents. Reliability and validity of the International Spinal Cord Injury Basic Pain Data Set gadgets as self-report measures. Prospective screening for blunt cerebrovascular injuries: analysis of diagnostic modalities and outcomes. Blunt cerebrovascular injury in cervical spine fractures: are more-liberal screening standards warranted Vertebral artery injuries associated with cervical backbone accidents: a evaluate of the literature. Incidence of vertebral artery thrombosis in cervical spine trauma: correlation with severity of spinal twine damage. Atlanto-occipital dislocation: a case research of survival with partial restoration and review of the literature. The value of retropharyngeal gentle tissue measurements in trauma of the grownup cervical backbone. Efficacy of postoperative radiograph for evaluating the prevertebral delicate tissue swelling after anterior cervical discectomy and fusion. The optimal radiologic method for assessing spinal canal compromise and cord compression in patients with cervical spinal twine 35 Initial Assessment (Including Imaging) of Cervical Spinal Cord Injury harm. Predicting the danger and severity of acute spinal cord damage after a minor trauma to the cervical spine. Radiographic clearance of blunt cervical spine injury: plain radiograph or computed tomography scan Computed tomography versus plain radiography to display for cervical spine injury: a meta-analysis. Value of complete cervical helical computed tomographic scanning in figuring out cervical backbone harm in the unevaluable blunt trauma affected person with multiple accidents: a prospective examine. Spiral computed tomography for the preliminary analysis of backbone trauma: a new commonplace of care Chance-type fractures of the thoracolumbar backbone: imaging evaluation in 53 sufferers. Neuroimaging in traumatic spinal wire harm: an evidence-based evaluation for medical follow and analysis. The position of magnetic resonance imaging within the administration of acute spinal twine harm. Reliability of magnetic resonance imaging in detecting posterior ligament complex harm in thoracolumbar spinal fractures. Magnetic resonance imaging within the analysis of spinal wire harm without radiographic abnormality in youngsters. Spinal twine damage after blunt cervical spine trauma: correlation of soft-tissue damage and extension of lesion. Computed tomography alone versus computed tomography and magnetic resonance imaging within the identification of occult injuries to the cervical backbone: a metaanalysis. Diagnostic capabilities of magnetic resonance imaging and computed tomography in acute cervical spinal column damage. Sixteen-slice multi-detector computed tomographic angiography improves the accuracy of screening for blunt cerebrovascular damage. Diffusion tensor imaging at 3 hours after traumatic spinal wire injury predicts long-term locomotor recovery. Magnetic resonance diffusion tensor imaging in sufferers with cervical spondylotic spinal wire compression: correlations between medical and electrophysiological findings. Increased sign intensity of the spinal twine on magnetic resonance pictures in cervical compressive myelopathy. Spinal fracture in patients with ankylosing spondylitis: cohort definition, distribution of accidents, and hospital outcomes. Multidetector computed tomography of cervical backbone fractures in ankylosing spondylitis. Emery Abstract Cranioskeletal traction is a treatment modality by which traumatic cervical fractures or dislocations can be decreased permitting reconstitution of the conventional cervical spine alignment. In doing so, the neural parts are freed of any ongoing compression from displaced vertebral or disc materials. Multiple units have since been invented which can be utilized to apply traction to the cervical spine; the two most commonly utilized units are the Gardner�Wells tongs and the halo apparatus.
In vitro susceptibilities of Candida albicans isolates to antifungal agents in Tokat arteria opinie 2012 buy genuine avalide on-line, Turkey blood pressure chart for children buy discount avalide on-line. National epidemiology of mycoses survey: A multicenter study of strain variation and antifungal susceptibility among isolates of Candida species blood pressure chart canada order avalide 162.5mg otc. Trends in candidemia and antifungal susceptibility in a college hospital in Northern Ireland 2001�2006 blood pressure medication and weight gain avalide 162.5mg low price. Fungemia at a tertiary care hospital: Incidence arteria zygomatica 162.5 mg avalide with amex, therapy blood pressure medication edarbi buy avalide 162.5 mg with mastercard, and distribution and antifungal susceptibility of causative species. Antifungal susceptibilities of Candida species causing vulvovaginitis and epidemiology of recurrent cases. Association between fluconazole susceptibility and genetic relatedness among Candida tropicalis isolates in Taiwan. Epidemiology of candidemia in a tertiary care centre of north India: 5-year examine. Multilocus sequence typing of Candida tropicalis shows clonal cluster enriched in isolates with resistance or trailing development of fluconazole. Candida nivariensis, an emerging pathogenic fungus with multidrug resistance to antifungal brokers. Outbreak of fungemia amongst neonates brought on by Candida haemulonii proof against amphotericin B, itraconazole, and fluconazole. Development of fluconazole resistance in a sequence of Candida parapsilosis isolates from a persistent candidemia affected person with extended antifungal therapy. Prevalent mutator genotype recognized in fungal pathogen Candida glabrata promotes multi-drug resistance. Candida tropicalis as a predominant isolate from scientific specimens and its antifungal susceptibility sample in a tertiary care hospital in southern India. Investigation of the first seven reported circumstances of Candida auris, a globally emerging invasive, multidrug-resistant fungus - United States, May 2013-August 2016. Evidence of genotypic variety amongst Candida auris isolates by multilocus sequence typing, matrix-assisted laser desorption ionization time-of-flight mass spectrometry and amplified fragment size polymorphism. Identification and typing of the emerging pathogen Candida auris by matrix-assisted laser desorption ionisation time of flight mass spectrometry. First report of Candida auris in America: Clinical and microbiological aspects of 18 episodes of candidemia. First hospital outbreak of the globally emerging Candida auris in a European hospital. Simultaneous emergence of multidrug-resistant Candida auris on three continents confirmed by wholegenome sequencing and epidemiological analyses. Trends in antifungal drug susceptibility of Cryptococcus neoformans isolates in the United States: 1992 to 1994 and 1996 to 1998. Fluconazole and itraconazole susceptibility of scientific isolates of Cryptococcus neoformans at a tertiary care centre in India: A want for care. Rates of antifungal resistance amongst Spanish clinical isolates of Cryptococcus neoformans var. In vitro antifungal actions of amphotericin B, 5-fluorocytosine, fluconazole and itraconazole in opposition to Cryptococcus neoformans isolated from cerebrospinal fluid and blood from sufferers in Serbia. Characterization of heteroresistance to fluconazole among scientific isolates of Cryptococcus neoformans. Antifungal susceptibilities of medical isolates of Candida species, Cryptococcus neoformans, and Aspergillus species from Taiwan: Surveillance of multicenter antimicrobial resistance in Taiwan program knowledge from 2003. Antifungal drug susceptibility of Cryptococcus neoformans from medical sources in Nairobi, Kenya. Increasing in vitro resistance to fluconazole in Cryptococcus neoformans Cambodian isolates: April 2000 to March 2002. Filamentous fungi in a tertiary care hospital: Environmental surveillance and susceptibility to antifungal medication. Epidemiological cut-offs and cross-resistance to azole drugs in Aspergillus fumigatus. Prospective multicenter worldwide surveillance of azole resistance in Aspergillus fumigatus. Vermeulen E, Maertens J, De Bel A, Nulens E, Boelens J, Surmont I, Mertens A, Boel A, Lagrou K. Zygomycosis in a tertiary-care most cancers middle in the period of Aspergillus-active antifungal therapy: A case- management observational study of 27 recent cases. Species distribution and in vitro antifungal susceptibility patterns of 75 scientific isolates of Fusarium spp. Activities of available and investigational antifungal brokers against rhodotorula species. Netsvyetayeva I, Swoboda-Kopec E, Sikora M, Jaworska-Zaremba M, Blachnio S, Luczak M. Trichosporon asahii as a potential pathogen in stable organ transplant recipients. Clade-related amphotericin B resistance amongst South African Candida albicans isolates. In vitro activities of 5-fluorocytosine against eight,803 medical isolates of Candida spp. Susceptibilities to amphotericin B and fluconazole of Candida species in Taiwan Surveillance of Antimicrobial Resistance of Yeasts 2006. Outbreak of Candida rugosa candidemia: An rising pathogen that may be refractory to amphotericin B remedy. Epidemiology and consequence of infections due to Aspergillus terreus: 10-year single centre experience. Emergence of a Candida krusei isolate with lowered susceptibility to caspofungin throughout remedy. Acquired echinocandin resistance in a Candida krusei isolate as a end result of modification of glucan synthase. Multiechinocandin- and multiazole-resistant Candida parapsilosis isolates serially obtained throughout remedy for prosthetic valve endocarditis. Differential in vitro exercise of anidulafungin, caspofungin and micafungin against Candida parapsilosis isolates recovered from a burn unit. Rapid improvement of Candida krusei echinocandin resistance during caspofungin remedy. Emergence of Candida glabrata isolates with lowered susceptibility to caspofungin and micafungin, however not anidulafungin. In vitro pharmacodynamics of anidulafungin and caspofungin against Candida glabrata isolates, together with strains with decreased caspofungin susceptibility. Epidemiology and danger elements for echinocandin nonsusceptible Candida glabrata bloodstream infections: Data from a big multisite population-based candidemia surveillance program, 2008�2014. The traits of Aspergillus fumigatus mycetoma development: Is this a biofilm Influence of lipid composition on the sensitivity of Candida albicans to antifungal brokers. A comparability of the sterol content of multiple isolates of the Candida albicans Darlington pressure with other clinically azolesensitive and - resistant strains. Accumulation of 3-ketosteroids induced by itraconazole in azole-resistant medical Candida albicans isolates. Phospholipid and sterol evaluation of plasma membranes of azole-resistant Candida albicans strains. The lipid composition and permeability to azole of an azoleand polyene-resistant mutant of Candida albicans. Antifungal agents: Mode of motion, mechanisms of resistance, and correlation of those mechanisms with bacterial resistance. In vitro low-level resistance to azoles in Candida albicans is associated with adjustments in membrane lipid fluidity and asymmetry Antimicrob Agents Chemother 2002;46(4):1046�1052. Altered P450 activity associated with direct selection for fungal azole resistance. Reduced susceptibility in laboratory-selected mutants of Aspergillus fumigatus to itraconazole as a outcome of decreased intracellular accumulation of the antifungal agent. A sterol-regulatory component binding protein is required for cell polarity, hypoxia adaptation, azole drug resistance, and virulence in Aspergillus fumigatus. Contribution of mutations within the cytochrome P450 14alpha-demethylase (Erg11p, Cyp51p) to azole resistance in Candida albicans. A new Aspergillus fumigatus resistance mechanism conferring in vitro cross-resistance to azole antifungals involves a mix of cyp51A alterations. In vitro evolution of itraconazole resistance in Aspergillus fumigatus entails multiple mechanisms of resistance. Resistance to itraconazole in Aspergillus nidulans and Aspergillus fumigatus is conferred by additional copies of the A. Alanio A, Denis B, Hamane S, Raffoux E, Peffault de Latour R, Menotti J, Amorim S, Touratier S, Bergeron A, Bretagne S. Azole resistance of Aspergillus fumigatus in immunocompromised patients with invasive aspergillosis. Sensitisation of an Azole-Resistant Aspergillus fumigatus Strain containing the Cyp51A-Related Mutation by Deleting the SrbA Gene. Coste A, Turner V, Ischer F, Morschhauser J, Forche A, Selmecki A, Berman J, Bille J, Sanglard D. Genotypic evolution of azole resistance mechanisms in sequential Candida albicans isolates. Genome-wide expression and site analyses of the Candida albicans Tac1p regulon. A gain-of-function mutation in the transcription factor Upc2p causes upregulation of ergosterol biosynthesis genes and elevated fluconazole resistance in a medical Candida albicans isolate. Mutations in transcription issue Mrr2p contribute to fluconazole resistance in scientific isolates of Candida albicans. Structural mechanism of ergosterol regulation by fungal sterol transcription factor Upc2. A Novel Zn2-Cys6 Transcription Factor AtrR Plays a Key Role in an Azole Resistance Mechanism of Aspergillus fumigatus by Co-regulating cyp51A and cdr1B Expressions. The development of fluconazole resistance in Candida albicans�an example of microevolution of a fungal pathogen. Correlation between rhodamine 123 accumulation and azole sensitivity in Candida species: Possible function for drug efflux in drug resistance. Multiple molecular mechanisms contribute to a stepwise development of fluconazole resistance in medical Candida albicans strains. Distinct patterns of gene expression related to growth of fluconazole resistance in serial Candida albicans isolates from human immunodeficiency virus-infected patients with oropharyngeal candidiasis. Torelli R, Posteraro B, Ferrari S, La Sorda M, Fadda G, Sanglard D, Sanguinetti M. Multiple resistance mechanisms amongst Aspergillus fumigatus mutants with high-level resistance to itraconazole. Posteraro B, Sanguinetti M, Sanglard D, La Sorda M, Boccia S, Romano L, Morace G, Fadda G. Mutation of G234 amino acid residue in Candida albicans drug-resistance-related protein Rta2p is associated with fluconazole resistance and dihydrosphingosine transport. Comparison of the efficacy of polyenes and triazoles against hematogenous Candida krusei an infection in neutropenic mice. Capsule enlargement in Cryptococcus neoformans confers resistance to oxidative stress suggesting a mechanism for intracellular survival. A practical variomics software for discovering drug-resistance genes and drug targets. Plasma Membrane Proteolipid three Protein Modulates Amphotericin B Resistance via Sphingolipid Biosynthetic Pathway. Flucytosine: A evaluation of its pharmacology, medical indications, pharmacokinetics, toxicity and drug interactions. The Aspergillus nidulans FcyB cytosine-purine scavenger is highly expressed during germination and in reproductive compartments and is downregulated by endocytosis. Papon N, Noel T, Florent M, Gibot-Leclerc S, Jean D, Chastin C, Villard J, Chapeland-Leclerc F. Flucytosine-fluconazole cross-resistance in purine-cytosine permeasedeficient Candida lusitaniae clinical isolates: Indirect evidence of a fluconazole uptake transporter. Cloning and expression of squalene epoxidase from the pathogenic yeast Candida albicans. Extra copies of the Aspergillus fumigatus squalene epoxidase gene confer resistance to terbinafine: Genetic approach to learning gene dose-dependent resistance to antifungals in A. A Phe389Leu substitution in ergA confers terbinafine resistance in Aspergillus fumigatus. Biological, biochemical, and molecular characterization of a new medical Trichophyton rubrum isolate immune to terbinafine. Terbinafine resistance mediated by salicylate 1-monooxygenase in Aspergillus nidulans. Specific substitutions within the echinocandin goal Fks1p account for reduced susceptibility of rare laboratory and medical Candida sp. A naturally-occurring Fks1p proline to alanine amino acid change in Candida parapsilosis, Candida orthopsilosis and Candida metapsilosis accounts for reduced echinocandin susceptibility. Overexpression of Sbe2p, a Golgi protein, results in resistance to caspofungin in Saccharomyces cerevisiae. The effect of the echinocandin analogue caspofungin on cell wall glucan synthesis by Cryptococcus neoformans. Biofilm formation by the fungal pathogen Candida albicans - growth, structure and drug resistance. Aspergillus fumigatus varieties biofilms with reduced antifungal drug susceptibility on bronchial epithelial cells.
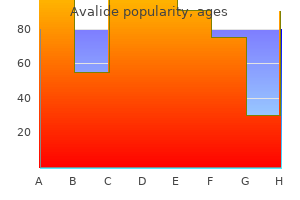
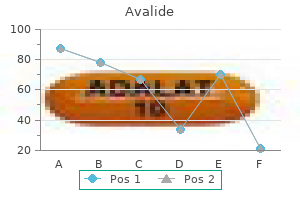
Epidemiology of Aortic Stenosis Valvular aortic stenosis blood pressure medication nightmares 162.5mg avalide with visa, as the most common valvular coronary heart illness hypertension 3rd stage generic 162.5 mg avalide amex, is often a illness of old age and a results of atherosclerotic changes blood pressure during pregnancy purchase avalide 162.5 mg with visa. It stays asymptomatic for many years in 50 % of cases and is associated with a good prognosis heart attack symptoms in women buy discount avalide on-line. If the disease turns into symptomatic arteria e veia generic avalide 162.5mg on line, the prognosis worsens to a 2-year survival fee of less than 50 % blood pressure medication raynaud's disease generic avalide 162.5mg line. Senile calcification: � the most common cause, especially amongst sufferers over 65 years of age. Calcification of a congenitally bicuspid aortic valve: � Associated with Turner syndrome. Rheumatic coronary heart disease: � � Frequently associated with rheumatic mitral valve illness. It has turn into rare in industrialized countries due to early antibiotic remedy of the accountable streptococcal infections. Classification of Aortic Stenosis A distinction should be made in accordance with localization: 1. Pathophysiology of Aortic Stenosis As the valve area decreases, the left ventricle must work tougher to pump blood all through the physique. In response to the elevated workload, the myocardium of the left ventricle hypertrophies; (muscles get larger when they work hard). In valvular aortic stenosis, the left ventricle has to use more power so as to preserve the cardiac output towards the pathologically increased strain gradient of the valve. In the lengthy term, diastolic dysfunction develops, resulting in pulmonary congestion and signs of coronary heart failure. Asymptomatic: � Patients with mild to average valvular aortic stenosis can remain asymptomatic for a very long time. High-yield: In asymptomatic patients, valvular aortic stenosis can result in sudden cardiac demise. Symptomatic � � � Symptoms develop late, when the aortic valve area < 1 cm�, and the stress gradient throughout the valve is 40�50 mmHg. Cardiovascular examination Palpation Left ventricular hypertrophy manifests as a visual and palpable heaving and widened apical impulse. Systolic crescendo-decrescendo murmur (diamond shape) is best heard at the proper 2nd intercostal space (first aortic area) and radiates to the carotid artery. Dynamic auscultation: � Valsalva and standing decreases venous return lower ejection fraction decreases murmur. Echocardiography � � the gold normal, non-invasive technique of assessing aortic stenosis etiology, severity and penalties. Examples are: � � Heart price controlling medication Afterload reducing drugs Note: Diuretics must be given with care to avoid decreasing cardiac output. Complications of Aortic Stenosis Complications of aortic stenosis are: � � � Arrhythmias Sudden cardiac dying Left ventricular failure Prognosis of Aortic Stenosis Rule of 5, 3, and 2. Congenital bicuspid aortic valve: � Most frequent in young adults and developed countries. Chronic aortic valve insufficiency subsequently causes an isolated left ventricular hypertrophy. With persistent insufficiency, however, the compliance of the ventricle decreases, in order that the conventional stroke volume can not be maintained. It additionally causes wide pulse strain (hyperdynamic circultation) due to wide distinction between systolic and diastolic blood strain. M�ller signal: Pulsation of the uvula that occurs throughout systole as a result of increased stroke quantity. Apex is often diffuse, displaced inferolaterally and characteristically hyperdynamic as a end result of eccentric hypertrophy and increased stroke volume. High-pitched, diastolic, blowing decrescendo murmur greatest heard at left third intercostal area (second aortic area) when sitting and leaning ahead. Dynamic auscultation: Squatting and hand grip elevated afterload elevated murmur. Occurs when the large amount of regurgitant blood strikes the anterior leaflet of the mitral valve, leading to premature closure of the mitral leaflets. Echocardiography Echocardiography is the gold normal for the assessment of underlying etiology, regurgitation fraction, and volume. Treatment of Aortic Insufficiency Conservative � Conservative medical therapy with observe up is really helpful in the: 1. Symptomatic remedy of coronary heart failure to relieve pulmonary congestion, corresponding to diuretics. Beta-blockers can utilized in sufferers with connective tissue issues, similar to Marfan syndrome, to slow aortic root dilatation and reduce danger of aortic issues. Beta-blockers to control coronary heart price and scale back sharing pressure as in aortic dissection. Try out the: Note: Surgery is indicated in Marfan syndrome with aortic root diameter > =50 mm regardless of the signs and Echo findings. Definition of Congestive Heart Failure Cardiac insufficiency refers to the lack of the center to supply the physique with regular cardiac minute quantity under regular end-diastolic pressure circumstances. Approximately 30 % of sufferers with persistent heart failure are readmitted inside 2 to three months. Most common causes of valvular cardiomyopathy are: � Rheumatic heart illness Specific causes of heart failure Systolic dysfunction 1. Constrictive pericarditis High-yield: Causes of reversible cardiomyopathy are: � � 2. Hypertrophic cardiomyopathy � � Viral myocarditis Metabolic acidosis (causes myocardial depression) Peripartum cardiomyopathy Tachycardia-induced cardiomyopathy Takotsubo cardiomyopathy (broken coronary heart syndrome) 2. Diastolic ventricular dysfunction � � Results from decreased ventricular compliance and elevated its stiffness, subsequently lowered diastolic ventricular filling, and cardiac output. This situation is mostly brought on by elevated afterload, as in hypertension. Note: It is troublesome to clinically differentiate between systolic and diastolic dysfunction. Aorta 2) Based on the side of the center Isovolumic strain decline Left atrium Diastole Depending on which chambers of the guts are affected, cardiac insufficiency could additionally be referred to as left ventricular heart failure, right ventricular coronary heart failure, or bilateral ventricular coronary heart failure (congestive coronary heart failure). Left-sided coronary heart failure Note: Diastolic dysfunction is simply identified by way of the observation of specific options utilizing Echocardiography. Poor organ perfusion, most commonly cardiorenal syndrome as a result of reduced renal filtration pressure. High-output coronary heart failure Occurs secondary to situations related to a high-output state, by which cardiac output is elevated to meet the demands of peripheral tissue oxygenation. Structural heart illness, in combination with cardiac insufficiency symptoms, is current. The release of natriuretic peptides, in addition to cardiac reworking and cardiac hypertrophy are additional compensatory mechanisms. Furthermore, cardiac insufficiency incessantly leads to a loss of contractility, regardless of pathological myocyte progress. Clinical Features of Congestive Heart Failure the symptoms of cardiac insufficiency are variable, relying on the severity of the insufficiency and the affected aspect of the heart. Left-sided heart failure Right-sided coronary heart failure Symptoms Dominant pulmonary symptoms Dyspnea Orthopnea Paroxysmal nocturnal dyspnea Pulmonary edema in acute severe instances Dominant venous congestion symptoms Lower limb swelling Abdominal distension Abdominal ache Jaundice Nausea and loss of urge for food (congestive gastropathy) Signs 1. Ascitis 133 Chapter 6: Congestive Heart Failure Symptoms embrace dyspnea on exertion or even at rest at extra advanced stages, bronchial asthma (cardiac asthma) and orthopnea, paroxysmal nocturnal dyspnea, and symmetric edema, particularly on the ankles, the tibia, and on top of the foot. Dyspnea and pulmonary edema are extra likely caused by acute left ventricular coronary heart failure, whereas proper ventricular coronary heart failure manifests as bilateral decrease limb edema, ascites, and gastrointestinal problems corresponding to tender hepatomegaly secondary to systemic venous congestion. High-yield: Biventricular coronary heart failure with options of left and right coronary heart failure is more likely than isolated failure of 1 ventricle. Diagnostics of Congestive Heart Failure Heart failure is mainly a clinical diagnosis. Laboratory investigations and different imaging modalities are used, mainly to assess the severity and reason for the situation. Assess pulmonary congestion: � Evidence of vascular redistribution (cephalization) � Kerley B traces � Pleural effusion Echocardiography Echocardiography is especially used for diagnosing the etiology and assessment of ventricular perform and hemodynamics. Diastolic function of the heart using Doppler alerts Note: the targets of therapy are to appropriate underlying trigger, enhance quality of life, forestall hospitalization, and extend life by neurohormonal blockade. Treatment of Congestive Heart Failure Several common measures in chronic coronary heart failure administration: � Correct modifiable risk factors of coronary heart failure, such as cessation of smoking and alcohol consumption. Chapter 6: Congestive Heart Failure Definition of Pulmonary Edema Acute pulmonary edema constitutes sudden accumulation of fluid in the lung tissue and alveoli because of either fluid redistribution as in hypertensive pulmonary edema, or fluid accumulation as in cardiogenic shock, because of pump failure. Pathophysiology of Pulmonary Edema the pathophysiology of pulmonary edema is based on an imbalance of fluid reabsorption and filtration. Increased pulmonary capillary strain shortly results in fluid build-up in the lungs and massively impairs gas change, which explains the respiratory failure. Lung compliance and important capability lower, airway resistance, and range in path length to gas exchange enhance. The pathophysiology of high-altitude pulmonary edema may be defined by a mix of a decrease in pulmonary oxygen content material, pulmonary vasoconstriction, and decreased alveolar strain. Clinical Features of Pulmonary Edema Depending on the stage of pulmonary edema, symptoms might embrace dyspnea, cough, thick mucus discharge, tachycardia, indicators of cyanosis, as well as restlessness. Note enlarged heart measurement, apical vascular redistribution (circle), and small bilateral pleural effusions (arrow). Diagnostics of Pulmonary Edema Aside from the medical historical past and medical image, moist rattling sounds are noticeable in cases of alveolar pulmonary edema which are, partially, already audible without the need for a stethoscope. Non-cardiogenic pulmonary edema the primary pathology is a direct or oblique insult to the pulmonary capillary membrane, secondary to inflammatory mediators which results in an increased permeability of the endothelial cell layer. She also gives a history of bilateral knee pain for five days which has now shifted to each ankles over the previous week. On common examination, patient is ill-looking with pallor and bilateral pitting edema of legs. On bodily examination, her apex beat is within the 5th intercostal area within the mid-axillary line with a outstanding apex beat, and bilateral basal crepitations are heard in chest examination. He first acknowledges having to catch his breath whereas gardening and is now unable to stroll up the stairs in his home with out stopping. He has sort 2 diabetes mellitus for 30 years, for which he takes metformin and sitagliptin. Definition of Acute Pericarditis Pericarditis is an inflammation of the pericardium ensuing from infection, autoimmune disease, radiation, surgery, or myocardial infarction, or is a post-surgical complication. It is manifested as fever, pleuritic chest ache that increases in the supine place, and an audible pericardial rub by auscultation. The serous pericardium is itself composed of two layers: the visceral pericardium connected to the outermost layer of the center, or epicardium, and the parietal pericardium which traces the within of the pericardial sac. The pericardial cavity between the visceral and the pericardial layers is filled with serous fluid. Epidemiology of Acute Pericarditis Acute pericarditis is diagnosed in about 1 in 1,000 hospital admissions. Purulent pericarditis (pericarditis with pus in the pericardial area, as the end result of bacterial infection) has become rare in the developed world due to the common use of antibiotics, but is still widespread within the creating world. An inflamed pericardium exhibits a polymorphonuclear infiltrate on microscopy and vascularization. Inflammatory signaling may stimulate the discharge of fluid that could result in effusion, or fibrinous reactants that would result in a constrictive complication. Tuberculosis, sarcoidosis, or fungal infections will show a granulomatous reaction with multinucleated large cells and epithelioid cells on microscopy. The accumulation of urea, a metabolic toxin, throughout the pericardial house leads to inflammation of the parietal and visceral layers. Clinical Features of Acute Pericarditis Symptoms � � � Patient often suffers from low grade intermittent fever, tachypnea, tachycardia, and diaphoresis. Persistent substernal chest pain (sharp or stabbing) that radiates to the trapezius or to the neck, and improves with leaning ahead, or is made worse in supine place, with coughing, or during inspiration. Signs � � Pericardial friction rub: a high-pitched scratching sound finest heard over the left sternal border throughout expiration whereas the patient is sitting up and leaning ahead. Colchicine may additionally be first-line or added to remedy regimen in circumstances of recurrent pericarditis. Treat the underlying condition � � Antibiotics to treat tuberculosis or different bacterial etiology. Post-myocardial infarct pericarditis is normally an indication of a large infarct and elevated mortality. Purulent pericarditis is associated with 40 % mortality, while tuberculous pericarditis is closer to 50 % mortality. She had a butterfly rash on her face, joint pains, fatigue, and elevated photosensitivity for a number of weeks now. Chapter 7: Pericardial Disease Definition of Constrictive Pericarditis Constrictive pericarditis is characterised by a thickened and scarred pericardial sac that lays across the coronary heart and prevents proper diastolic filling. The inset image is an enlarged cross-section that exhibits the infected and thickened layers of the pericardium. Approximately 10 % of acute pericarditis instances progress to constrictive pericarditis. High-yield: Tuberculosis is considered the most common reason for constrictive pericarditis In the developing world. Etiology of Constrictive Pericarditis In the previous, constrictive pericarditis was related to bacterial pericarditis and purulent pericarditis. Constrictive pericarditis is often iatrogenic following open coronary heart surgical procedure or radiation remedy for the therapy of mastocarcinoma and other cancers. Radiation-induced constrictive pericarditis often presents 10-years publish remedy. If this ends in active group, the parietal and visceral linings will turn out to be thickened and fuse. Note: Pulsus paradoxus is a more than 10 mmHg drop in systolic blood stress throughout inspiration.
Syndromes
Lymphoma
Pancreatitis
You may also be given medicines may also be used for the same purpose.
Tuberculosis
Myxedema
Sinus infection (sinusitis)
Dementia that becomes worse over time
Meningitis - cryptococcal
Triazoles may be subdivided into first 457 458 Newer antifungal agents in pediatrics (fluconazole and itraconazole) and second technology (voriconazole heart attack zone buy generic avalide 162.5mg line, posaconazole blood pressure pediatric buy cheapest avalide and avalide, and isavuconazole) brokers heart attack demi lovato discount avalide 162.5 mg free shipping. It is much less clear if therapeutic drug monitoring is required throughout major azole prophylaxis prehypertension 133 cheap generic avalide uk, though low ranges have been associated with a better likelihood of breakthrough an infection blood pressure good buy avalide 162.5mg with mastercard. It has potent exercise towards a broad spectrum of clinically related fungal pathogens blood pressure normal low avalide 162.5 mg otc, including Aspergillus, Candida, Cryptococcus, and some less frequent molds [3] (Table 28. In adults, its oral bioavailability is bigger than 90%; however, its oral bioavailability is more modest in youngsters, ranging from 44%�65% [4,5]. Pharmacokinetic modeling means that this distinction could be accounted for by intestinal first cross metabolism occurring in youngsters but not adults [6]. Voriconazole undergoes intensive hepatic metabolism by the cytochrome P450 system and dose adjustment is really helpful in people with hepatic impairment. About 5% of white individuals and 15%�20% of non-Indian Asians have a sluggish metabolizer phenotype. In addition to genetic variation in voriconazole metabolism, there are essential age-related differences with implications for pediatric dosing. In distinction to adults and older kids, in whom voriconazole metabolism is nonlinear (resulting in marked increases in drug exposure related to comparatively small adjustments in dose), younger children have linear metabolism and subsequently require much larger proportional doses to obtain adequate drug exposure. An open, multi-center research investigated the security, tolerability, and pharmacokinetics of intravenous voriconazole in immunocompromised pediatric sufferers [11]. This examine included a single-dose-study of eleven patients ages 2�11 years (mean age 5. Each child received both 4 mg/kg/dose adopted by 6 mg/kg/dose or 6 mg/kg/ dose followed by 8 mg/kg/dose. Each child additionally acquired at least two different doses in escalating order after which was switched to oral voriconazole. Interestingly, the bioavailability of oral voriconazole was decrease (65%) than seen in grownup sufferers (96%) [14]. This examine additionally demonstrated a excessive interpatient pharmacokinetic variability, as has been reported for studies concerning voriconazole drug level monitoring, however no important variations had been seen in the 2�6 yr vs. However, this pharmacokinetic research raised a number of important factors that remain inconclusively investigated. Given the substantial inter-individual variability in voriconazole pharmacokinetics, therapeutic drug monitoring of voriconazole ranges is recommended to gauge adequacy of remedy and to keep away from potential toxicities; target trough concentrations between 1 and 5 g/L are recommended [16]. With linear pharmacokinetics in youngsters, clinicians have a wider therapeutic window with which to safely increase the voriconazole dose. These dosing issues are particularly problematic with the known differences in metabolism throughout affected person subpopulations and the concerns of a lack of ordinary effective voriconazole degree objectives. For kids, voriconazole is available as an orangeflavored suspension (40 mg/mL). A widespread apply in pediatrics is to crush tablets and administer them to pediatric sufferers by way of a gastric or duodenal tube. A study examined the bioavailability of crushed or entire voriconazole tablets in an open-label, randomized, two-way crossover study in 20 health volunteers [17]. While there was a slightly faster time to most serum focus with the crushed tablets (0. Less widespread but critical toxicities embody neurotoxicity with outstanding visible hallucinations [21], which is related to serum trough levels above 5. Voriconazole produces some distinctive transient visual field abnormalities in about 10% of adults and youngsters. In some rare long-term (mean of 3 years of therapy) circumstances, this voriconazole phototoxicity has developed into cutaneous squamous cell carcinoma [22]. Clinical experience and pediatric knowledge A multi-center, randomized, open trial compared the result of patients receiving either intravenous voriconazole or amphothericin B deoxycholate for major therapy of invasive aspergillosis [23]. The overall response price at 12 weeks showed statistically considerably more full and partial responses in patients treated with voriconazole (52. Voriconazole-treated sufferers also had a higher survival fee than Amphotericin B�treated patients (70. Therefore, no agency conclusions can be made on the prevalence of voriconazole over amphotericin B in this age group. A minority of 52/144 (36%) patients in the voriconazole group and a majority of 107/133 (80%) patients within the amphothericin B group received one other licensed antifungal therapy apart from their major examine drug, resulting in a smaller ultimate group of sufferers receiving only voriconazole or solely amphothericin B. Patients receiving voriconazole as preliminary remedy and then switching to another antifungal drug nonetheless had a higher rate of full and partial responses than patients who obtained amphothericin B as initial drug adopted by another antifungal agent (48% vs. An additional open examine confirmed these promising data by administering voriconazole as main (52%) or salvage remedy (48%) to 116 sufferers with invasive aspergillosis [25]. Up to 48% of the sufferers demonstrated a complete or partial response, whereas in 21% the disease was stable and in 31% failed. The results of those medical research have led consultants to suggest voriconazole as the preferred antifungal against invasive aspergillosis [26]. In one other multicenter research of 422 sufferers with candidemia, voriconazole was as efficacious as amphothericin B adopted by fluconazole [28]. Moreover, voriconazole also demonstrates similar success rates and less breakthrough fungal infections compared to liposomal Amphotericin B in sufferers with neutropenia and chronic fever [29]. The largest pediatric research reported on fifty eight youngsters (ages 9 months-15 years, imply 8. Responses to the therapy with voriconazole were full or partial in 26 (45%), steady in four (7%) and failed in 25 (43%) patients. In a subsequent case collection, voriconazole was utilized as salvage therapy in 7 kids (age vary 2�13 years, median 5 years) with invasive aspergillosis [31]. Complete and partial response was observed in each of two patients, steady response in 1 affected person and failure of the voriconazole therapy in 2 sufferers. There are ongoing issues concerning the impact of voriconazole on the creating retina in neonates because of the well-documented visual disturbances in pediatric and adult patients. Posaconazole has wonderful exercise against both yeast and mold infections, particularly together with exercise in opposition to zygomycosis where voriconazole has no antifungal efficacy [32]. The bioavailability of posaconazole will increase significantly when administered in divided doses. One research showed the best bioavailability of posaconazole in fasting wholesome volunteers receiving 800 mg/day divided in 4 doses compared to 800 mg/day divided in either 1 or 2 doses [34]. When administered in the fed state, 800 mg/day divided in two doses gave comparable serum levels to dosing 4 occasions day by day and is extra sensible for compliance. Another examine reported on posaconazole in 98 adult patients with febrile neutropenia or refractory fungal infections [35]. Posaconazole has dose-proportional pharmacokinetics as much as 800 mg/day, and has a big apparent volume of distribution with sluggish elimination, suggesting an in depth distribution into tissues. Posaconazole is metabolized by glucuronidation and primarily eliminated via the fecal route. Posaconazole is an inhibitor of Cyp3A4 metabolism and P-glycoprotein transport and is topic to drug interactions with substrates for these pathways, such as calcineurin inhibitors or benzodiazepines. The most common drug-related opposed occasions are gastrointestinal (nausea, vomiting, abdominal pain) and hepatic (elevated hepatic enzymes and alanine aminotransferase) [37,38]. Serum samples obtained on 12 pediatric (ages 8�17 years) and 194 grownup (ages 18�64 years) patients from a multicenter, part three, open-label research of patients with invasive fungal infections refractory to normal antifungal therapies have been analyzed as preliminary comparisons of grownup versus youngster pharmacokinetics [39]. All patients obtained a upkeep dose of 800 mg/day in divided doses except 1 pediatric affected person who obtained 400 mg/day as a divided dose on the day of pattern assortment. The mean plasma concentrations of posaconazole in 462 Newer antifungal agents in pediatrics youngsters and adults were 776 ng/mL (median 579 ng/mL; range eighty five. One limitation with this study is that whereas the age vary of the 12 pediatric sufferers was 8�17 years, it consisted of a single eight year-old patient, a single 10-year old affected person, and all other sufferers had been 12 years old. This skew toward youngsters may explain the outcomes much like grownup dosage findings. Clinical experience and pediatric data In grownup patients with severe graft-versus-host illness posaconazole was as effective as fluconazole as antifungal prophylaxis, however extra effectively prevented invasive aspergillosis in addition to breakthrough invasive fungal infections and decreased deaths because of invasive fungal infections [40]. Moreover, in adult sufferers with neutropenia posaconazole was superior to either fluconazole or itraconazole in stopping invasive fungal infections (2% vs. It demonstrated comparable efficacy to fluconazole within the remedy of oropharyngeal candidiasis, with significantly decrease rates of relapse [42]. Posaconazole showed a survival benefit over historic controls in treating invasive aspergillosis as salvage antifungal therapy [43], and demonstrated successful fee of 72% in treating invasive aspergillosis that was refractory to voriconazole [44], however has not been examined as main therapy. A evaluate of 96 case reports describing posaconazole as a mixture or second-line remedy for mucormycosis discovered an approximately 70% price of complete or partial response, however the true success price is in all probability going decrease due to publication bias [45]. Segal and colleagues reported on 7 pediatric (ages 9�18 years) and 1 adult patient (age 36 years) with persistent granulomatous disease and invasive filamentous fungal infections who received posaconazole as salvage therapy [37]. Treatment with posaconazole led to a whole response in 7/8 grownup including 6/7 pediatric patients. Importantly, in that examine, the prior antifungal drug was voriconazole in 7/8 patients and was discontinued because of failure (n = 6) or intolerance (n = 1). Overall, 79% of patients had a complete or partial response while all 3 pediatric patients have been treated successfully (1 full response and a couple of partial responses). A subsequent multicenter retrospective survey of 15 kids age 3�17 years with invasive fungal infections refractory to first-line remedy demonstrated complete or partial response to remedy in 9 sufferers and no extreme antagonistic occasions, though gentle opposed events were reported in eleven sufferers [48]. Posaconazole may have an necessary function in antifungal administration sooner or later, however devoted pediatric clinical research, each to define the optimum dosing in kids and for comparative efficacy, have but to be performed. The pediatric oral suspension dose recommended by some experts for treating invasive illness is eighteen mg/kg/day divided three instances day by day, but the true answer is likely larger and serum trough stage monitoring is really helpful. A research with a new pediatric formulation for suspension, basically the pill kind that is ready to be suspended, is underway. Similarly, in adult sufferers, the extended-release tablet is dosed as 300 mg twice daily on the primary day, after which 300 mg once daily beginning on the second day. In grownup sufferers, the utmost quantity of posaconazole oral suspension given is 800 mg per day due to its excretion, and that has been given as 400 mg twice every day or 200 mg four times a day in severely sick sufferers because of findings of a marginal increase in exposure with extra frequent dosing. Like voriconazole and itraconazole, trough levels should be monitored, and most specialists feel that posaconazole levels for remedy must be at least larger than 700 ng/mL (0. It has a broad spectrum Caspofungin 463 of activity including Candida, Cryptococcus, Aspergillus, and the Mucorales. The prodrug, isavuconazonium, is quickly cleaved by plamsa esterases to isavuconazole. Oral bioavailability is 98% with low intersubject variability and no clinically important meals effect. It is water soluble with excessive protein binding, a large quantity of distribution indicating probably excessive tissue penetration. It exhibits doseproportional pharmacokinetics with reasonable deviation from linearity. Elimination is primarily although hepatic metabolism; its prolonged half-life permits once daily dosing following preliminary loading doses [49,50]. Isavuconazole is each a substrate and an inhibitor of Cyp3A4 and is therefore topic to clinically significant drug-drug interactions with Cyp3A4 substrates, inhibitors or inducers. The most frequently reported adverse occasions in scientific trials have been gastrointestinal symptoms, headache, elevated hepatic enzymes, hypokalemia, dyspnea, cough, peripheral edema, and back pain. The general incidence rates of adverse events were related between isavuconazole and voriconazole, however drug-related adverse occasions have been much less frequent with isavuconazole, and the frequency of dermatologic and visual antagonistic events was decrease with isavuconazole [51]. While the 3 clinically obtainable echinocandins, every individually have some unique and important dosing and pharmacokinetic parameters, especially in kids, efficacy is generally equivalent. Opposite the azole class, the echinocandins are fungicidal towards yeasts but fungistatic in opposition to molds. The fungicidal activity towards yeasts has elevated the echinocandins to the popular therapy in opposition to invasive candidiasis. Echinocandins are thought to be finest utilized against invasive aspergillosis only as salvage therapy if a triazole fails or in a affected person with suspected triazole resistance, but not as main monotherapy towards invasive aspergillosis or any other mildew an infection. Improved efficacy with combination remedy with the echinocandins and triazoles in opposition to Aspergillus infections is unclear, with disparate results in a number of smaller research and a definitive clinical trial demonstrating minimal benefit over voriconazole monotherapy in only sure affected person populations. Some specialists have used combination therapy in invasive aspergillosis with a triazole plus echinocandin solely in the course of the preliminary section of ready for triazole drug ranges to be appropriately excessive. Clinical experience and pediatric data In a section 2 randomized controlled trial comparing three isavuconazole oral dosing regimens (including a as quickly as weekly regimen) to oral fluconazole for therapy of esophageal candidiasis in immunocompromised patients, all three regimens were non-inferior to fluconazole [52]. Rates of endoscopically confirmed remedy have been 95%�98% for the isavuconazole regimens and 95% for fluconazole. A part three randomized controlled trial compared isavuconazole to voriconazole for treatment of invasive aspergillosis and other invasive mould infections in 516 immunocompromised adults [51]. On the primary endpoint of all-cause mortality at 6 weeks, isavuconazole was non-inferior to voriconazole, with 18. Overall remedy success on the end of therapy was also comparable between teams. An open-label non-comparative trial evaluated isavuconazole for treatment of 37 patients with confirmed or probable invasive mucormycosis, both as primary or salvage remedy [53]. All-cause mortality at 6 weeks was 38% and overall response at finish of remedy was 31%; in gentle of the severe natural history of invasive mucormycosis, this trial helps clinical efficacy of isavuconazole in remedy of mucormycosis. An additional scientific trial is underway evaluating isavuconazole for treatment of invasive candidiasis. Caspofungin is primarily excreted by the liver and not metabolized by the cytochrome 464 Newer antifungal agents in pediatrics P450 enzymes [58,59]. Tissue distribution accounts for an initial rapid decline in plasma ranges, and subsequently the drug undergoes sluggish hepatic metabolism through hydrolysis and N-acetylation. The drug additionally undergoes spontaneous degradation; these processes together account for a terminal halflife of 27 to 50 hours. Caspofungin shows linear pharmacokinetics after single dosing however modest nonlinearity after a number of dosing [59]. In adults, a loading dose of 70 mg on the first day, adopted by a upkeep dose of 50 mg day by day is beneficial [59]. However, in sufferers with moderate hepatic insufficiency, reduction of the upkeep dose to 35 mg/day after the preliminary 70 mg loading dose is recommended [61].
Buy discount avalide 162.5mg. Eddie Bravo Quits Drinking Alcohol.